WAS POLIO ERADICATED?
*You’re about to read some of the highlights of the history of the polio vaccine. By no means is this the whole story. We are hoping this article will open the door to start shining a light on what happens when political policy merges with medical science. When we can step back and see that public health recommendations can be political decisions dressed up in a lab coat, that history is part of your informed consent or refusal.
Do you know people who say vaccines eradicated polio? Is that true? Is it possible?
When people contemplate the necessity of vaccines, polio is usually the one they point to. They tell a story of a terrifying time when young children would be thriving one day, and paralyzed the next. Polio did not discriminate and it didn’t follow the rules: it struck the young more than the old, it surged in warm weather instead of cold, and didn’t care about your zip code. Polio didn’t follow the typical rules for sickness people knew. It struck places that were not impoverished or unsanitary. No one felt safe from the disease. Coffin-like ”iron lungs” merged man with machine, saving lives with the power of science, and leaving an indelible impression on the minds of people, in a way the modern-day ventilators do not.
After the devastation of World War II (WWII) ended in 1945, a different type of war was exploding on American soil — polio cases were surging. Fear gripped the country, demanding action in a time where science was suddenly revered as savior. In both World Wars I and II, technology such as radio communication, nuclear weapons, influenza shots, and antibiotics were new and used strategically to win the wars. Science was seen as a way to secure freedom.
Many people are aware of the “space race” or the “arms race” of the Cold War that started after WWII between the U.S. and the Soviet states, but few are aware that this technological showdown included public health as well — specifically, the polio vaccine.
As countries were picking up the pieces after WWII, public health was a battleground for global dominance. A new cold war took center stage between the U.S. and allies with free markets and democratic-style governments, and on the other side, socialism championed by the USSR. Very broadly, WWII ripped through countries both physically and ideologically. When it came time to put the world back together, some believed individuals were the core of a society served by government, and others believed the people should be subservient to the collective. This debate echoes still in the decades-long debate about “socialized” medicine in the United States.
A healthy population became the bellwether of the Cold War between capitalism or socialism, because sick people can’t work for themselves or for the state. Sickness and poverty were tied together. “[T]he U.S. State Department regarded medical and economic assistance for developing countries as tools to repel enslaving Soviet influence by contributing to liberating wars or crusades against disease.”[1] In short, the U.S. believed that by eradicating disease, they would also eradicate communism. And so, with polio surging around the globe, a medical solution was expected to move “at the speed of science” (to use today’s terms).
Let’s start from the beginning.
HOW WAS THE POLIO VACCINE DEVELOPED?
The first mass-produced polio vaccine was created by Jonas Salk, who had worked under Dr. Tommy Francis with the U.S. Army Epidemiological Board. Salk and Francis worked together to create the first influenza vaccines.
Jonas Salk was known to play fast and loose with the conventions of science. This contributed to his success in the scientific community because his innovation caught the eye of the National Foundation for Infantile Paralysis, (Later known as the March of Dimes), top funders of polio vaccine research. This non-governmental organization came from work started by Franklin Delano Roosevelt (FDR) and passed on to associate Basil O’Connor as FDR regained his political footing after paralysis attributed to polio took him out of the political sphere. Amidst a national cry for a medical solution as parents feared their children could be stricken, the National Foundation recruited Salk as lead scientist for the polio vaccine hunt. All the other scientists were saying it would take years to come up with a vaccine. Salk had a different technique.
The Salk vaccine was an injectable shot containing a “killed” (now known as inactivated) virus and it faced a lot of opposition in the scientific community. Many scientists believed it was not possible to create an effective or safe vaccine by using chemicals to “kill” a virus just enough for it to not create a full-on disease, but leave it intact enough to stimulate an immune response. And controversy swirled around the effectiveness of a shot that would go into the bloodstream, rather than following the scientific consensus of the natural way people became afflicted with polio, (through their gut). But fear of the worst-case scenario of permanent paralysis or death, and desperation to find something to stop it, had parents lining up to volunteer their children for field trials. Ensuing demand for the vaccine product led to a quick-and-dirty shot that became available in 1955 and harmed hundreds of thousands of people, mostly children.
Salk began testing his vaccine in small field trials. In 1952, he quietly experimented on over 150 children and deemed the shot a success.[2] The first field trial for the Salk polio vaccine was held in 1954. Parents volunteered their children to be “polio pioneers,” becoming the first vaccinated with an experimental shot.
Because there were so many questions about the safety of the shot, the National Foundation brought in Salk’s old mentor Tommy Francis to head the group tasked with determining the safety of the polio vaccine. Francis, as you may remember from Shining a light on influenza vaccines, was known for his integrity. Bringing him in to bless this vaccine gave it credibility in the scientific community that couldn’t be bought.
THE CUTTER INCIDENT
In 1955, the Salk vaccine was celebrated as a massive success. It was labeled safe and effective and ready for mass inoculation. Public health authorities immediately licensed six pharmaceutical companies to produce the vaccine. Among the chosen companies was Cutter Laboratories located in Berkeley, California.
But something horrible was happening during the manufacturing of the Salk vaccine. Manufacturers were having trouble scaling up Salk’s vaccine from his instructions. The value and validity in scientific discovery comes from others being able to replicate findings. And when it comes to selling that finding, that replication needs to be not just reproducible, but also scaled up for sales. Salk vaccine production required that poliovirus be “killed” with formaldehyde. Unfortunately, that step of the process relied on an assumption that was made in Salk’s lab that didn’t work in mass production, leaving manufacturers in the dark about the true nature of what was in their shots. Inevitably, in the first mass rollout of the Salk vaccine, many people were hurt. It’s hard to get an exact number on adverse reactions, but it’s safe to say tens of thousands of children suffered headaches, fatigue, muscle weakness and stiffness, as well as other symptoms associated with polio. Approximately 200 children were paralyzed from the Salk vaccine initial rollout, and at least 10 are known to have died as a direct result.
According to vaccine expert Dr. Paul Offit, in his book “The Cutter Incident,” “After receiving Salk’s vaccine, forty thousand children developed headaches, neck stiffness, muscle weakness, and fever; about two hundred were permanently and severely paralyzed; and ten died….Children were getting polio even though polio season was still a few months away. And children given Salk’s vaccine were spreading polio to others.”[3]
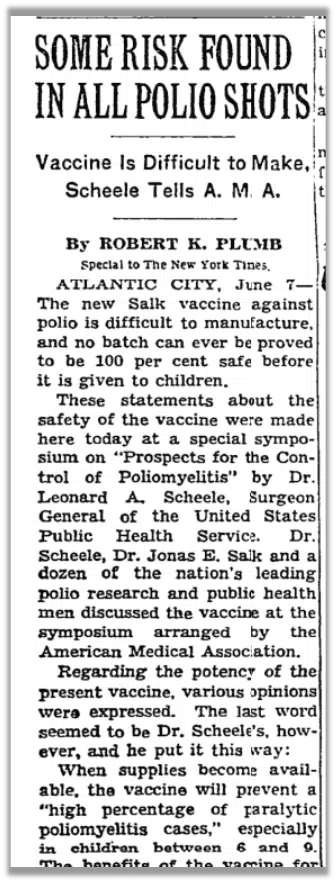
Many of the injuries were publicly traced back to the Cutter Laboratory, and therefore this was the company highlighted for safety concerns, but there is evidence the contamination was widespread among all the labs. The Cutter Incident, as it came to be called, put vaccine injury in the spotlight for a brief moment in time, with questions about risk making the front page of the New York Times in 1955.
The company was not shut down. It was eventually able to continue making the vaccine. But remember, there were five other labs manufacturing this vaccine and they all had the same issue. But it was only Cutter that was sued and ordered to pay damages for breach of warranty, having claimed that the vaccine was safe when it manifestly wasn’t.
There’s no doubt that the Cutter Incident, in which 400,000 humans (mostly children) were given the first mass-produced polio vaccine, was a result of rushed science.
According to historian Arthur Allen, author of a book titled “Vaccine,” after the Cutter Incident, the federal government “established a Polio Surveillance Unit at the Communicable Disease Center that would track cases of vaccine-related and wild polio. From this start the CDC vastly expanded its surveillance of infectious disease in the United States.”
WAS THE POLIO VACCINE CONTAMINATED WITH A CANCER-CAUSING SUBSTANCE?
Yes. We’ll let the CDC speak on this one.

“Because of research done with SV40 in animal models, there has been some concern that the virus could cause cancer in humans.”
The CDC has an admission on its website as of March 2023 that “From 1955 to 1963, an estimated 10-30% of polio vaccines administered in the U.S. were contaminated with simian virus 40 (SV40).”[4]
The government, the National Foundation, and scientists involved with production of the polio vaccine were all aware of the potential contamination of all the vaccines. Due to the nature of production using crude methods to cultivate the virus in monkey kidneys at a time when the poliovirus had not yet even been seen under a microscope, it was common knowledge among the scientific community that it was impossible to filter out or kill whatever may be coming from the monkeys that was unintended and unknown. When one looks at debates and discussions of the time, arguments take contamination as a basic fact, but people disagreed on how much that mattered — in other words, whether people would be harmed by unavoidable toxins or monkey viruses. In fact, SV40 got it’s name in a very methodical manner: SV stands for simian virus and 40 tells us it is the fortieth virus that was found and labeled. It wasn’t the last.
One intrepid public health researcher, Dr. Bernice Eddy, tried in vain to warn the scientific community of her findings that there was some agent in monkey cultures that could cause cancer in lab animals and therefore potentially in humans as well.[5] When she brought her information to light, her supervisors in the federal government blocked her ability to publish her findings or speak at conferences. They did not fire her, but instead kept her on board and stifled her research by moving her out of her lab and effectively silencing her.
Interestingly, her work eventually did come to light when Merck scientist Maurice Hilleman tried to discredit the Sabin vaccine with the unspoken knowledge that monkey cultures inevitably have contamination. His announcement of this to a wide audience was calculated to knock out competition because his lab was working on a Salk-like killed vaccine. His theory was that the formaldehyde that killed the poliovirus enough in their shots would also kill the monkey virus, whereas Sabin’s live virus vaccine did not use that step and therefore would be contaminated. Unfortunately for Dr. Hilleman, after blowing the trumpet about SV40, the Salk injectables were tested by alarmed researchers and found to be contaminated as well.
SEEDS OF GLOBAL PUBLIC HEALTH: THE SABIN ORAL POLIO VACCINE
It took a few more years before an oral polio vaccine (OPV) was finalized. It took longer to create, but it was quickly accepted around the world as superior in efficacy, administration, and cost.
Albert Sabin believed the Salk vaccine was ineffective at best, dangerous at worst. In addition to safety concerns, its efficacy was questionable, as polio outbreaks continued to rage — even increasing after the vaccine was introduced. Massachusetts had its biggest outbreak of polio after vaccine rollout. (It makes one think of Barnstable, Massachusetts’ explosive outbreak in 2021 where the CDC estimated 74% of those with COVID were “fully vaccinated.”[6])
While Salk’s vaccine moved like wildfire through the United States, Sabin continued his work. He believed an injectable vaccine would not work because the virus moved through the gut (an enterovirus) and therefore needed to be administered the same way one would naturally encounter it: through the stomach.
Because of the disasters of the Salk vaccine, the U.S. government and the National Foundation did not want to take a chance on a new formulation. So when Sabin finally announced he was ready for field trials, the U.S. government said no.
Sabin was determined. He turned to his Russian ties. The Soviets welcomed him with open arms and ultimately licensed his OPV for use. Sabin’s vaccine was easier to administer (and so more people would get it, and faster). It cost less to produce, and the scientific consensus was that it was safer and more effective than the Salk vaccine.
The U.S. had no choice but to switch production from the injectable killed virus shot to Sabin’s oral concoction. It was not acceptable to have a global perception that Soviet socialized medicine was superior to the free market in the U.S.
Interesting to note, the Cold War was the crucible in which the World Health Organization was formed. The concepts that socialized medicine held that health was a product of social and environmental conditions (which we would now call “Social Determinants of Health”), and that innovations should not generate profit, were in striking opposition with the U.S. view that medical technology spurred on by profit would stop the spread of disease and save the day no matter where it was used.
As recounted by WHO historians: “In 1949, a communist delegate to the World Health Assembly denounced the agency as the battleground of ‘two opposing points of views…[that of the Soviet Union] standing for the interest of humanity, which demands that the attainment of medical science should serve the whole human race…while the capitalist camp represent the interest of a minority who consider science as a source of income and a weapon of war.’ “[7]
WAS POLIO ERADICATED?
WHAT IS POLIO?
When you ask someone what polio is today, you will likely get an answer something like, it’s a virus that causes paralysis. But the term polio, like influenza, started as a catch-all to describe a collection of symptoms. In the 1800s and early 1900s, most people knew it as “infantile paralysis” rather than polio.
The word poliomyelitis describes an inflammation of the marrow of the spinal column. Its roots are in the Greek words polios (grey) and muelos (matter), with the medical suffix –itis meaning inflammation.
Dr. Suzanne Humphries and medical historian Roman Bystrianyk explain the landscape of what was considered polio in their extensively cited book, “Dissolving Illusions.” They point out that testing for a specific poliovirus was not common before 1958, so a polio diagnosis was a subjective observation and assessment by a doctor. Many diseases and toxins can present in a fashion that someone might label as polio, including hand, foot, and mouth disease; lead poisoning, Guillain-Barre syndrome, transverse myelitis, cerebral palsy, muscular dystrophy, DDT and arsenic toxicity, and other “stomach bugs” known as enteroviruses.
POLIO STATISTICS ARE UNRELIABLE
A federal Public Health Service pamphlet from 1977 gave parents this warning, “The fact is, however, that while polio cases may be few in number today, the outlook for tomorrow is ominous.”[8]
But what were those statistics and how certain are we of their accuracy? From the start of trying to quantify polio cases, there’s been difficulty counting. One reason is because when the vaccines were rolled out in the early 50s, with surveillance systems in place, the top medical minds in the world were still unsure how polio was contracted and whether a child could have “polio” but show no signs, or show only signs of something like a common flu.
Interestingly, the authors uncovered a quote from a 1969 discussion of the polio vaccine at the 120th annual meeting of the Illinois State Medical Society that reveals doctors were incentivized to make a diagnosis of polio.[9] While describing statistical questions about the “misleading way” polio was reported and recorded, Dr. Bernard Greenberg, a highly respected and published statistician, noted that a doctor diagnosing polio was “doing his patient a service by way of subsidizing the cost of hospitalization and was being community-minded in reporting a communicable disease.” Presumably, Greenberg was referring to the all-expense-paid, treatment-for-life promised to polio victims by the National Foundation for Infantile Paralysis.
Experts and historians disagree about how many people had “polio,” how many cases were paralytic, and whether there were enough cases to count as an epidemic at different times.
In a transcript of this historic discussion, titled “The Present Status of Polio Vaccines,” a footnote explains the wordsmithing that affected statistics of polio epidemics because “prior to the introduction of the Salk vaccine the National Foundation defined an epidemic as 20 or more cases of polio per year per 100,000 population. On this basis there were many epidemics throughout the United States yearly.” But after the introduction of the vaccine, the definition increased the threshold for cases before an epidemic would be found, from 20 to 35. “The present higher rate has resulted in not a real, but a semantic elimination of epidemics.”[10]
Dr. Greenberg became outspoken about his questions surrounding the data used to promote the Salk vaccine. His words from ”The Present Status of Polio Vaccines” were quoted in testimony to Congress in 1962:
Greenfield further explained that the diagnostic criteria for paralytic polio changed when the vaccine was introduced. Prior to the Salk vaccine licensure, most medical professionals used the WHO criteria for determining whether symptoms pointed to polio. All that required was observed paralysis of one or more muscle groups, detected on two exams at least 24 hours apart. After the vaccine, medical professionals shifted their diagnostics to conform more with the Salk field trials, which greatly expanded the timeframe for sustained paralysis from one day to 60 days. Think about that: What effect would that have on data?
In 1954, if a person experienced paralysis temporarily for 24 hours they were considered a paralytic case. The next year that same person would have to have persistent paralysis for two months to be considered having the same exact diagnosis. How would that change the number of people considered to have paralytic polio? Logically, the number of cases would decline simply because of the way the disease was defined. This would be the same as looking around your house for seating for a party and deciding anything a person can sit on is a seat and counting that for your guests, in contrast with a formal dinner where your seats must have four legs and fit around a dining room table. Your house is the same, your furniture is the same, but the amount of party guests is drastically different, simply because of the way you are defining a chair. According to Greenfield, these diagnostic criteria change effectively means, “in 1953 we started reporting a new disease, namely paralytic poliomyelitis with a longer lasting paralysis.” In today’s terms, would the public call this long-haul paralytic polio, and would it be considered a different disease (and therefore medically coded differently) from the initial polio diagnosis?
Researcher Janine Roberts further describes the changes in diagnoses, not just of polio, but in other diseases with the same symptoms in her book “Fear of the Invisible.” She found evidence that “all cases of polio occurring within 30 days of vaccination were to be recorded, not as possibly caused by the vaccine, but as ‘pre-existing.’ This regulatory change also ensured that far fewer cases of vaccine failure would be recorded.”[11]
After observing waning effectiveness and the failure of multiple boosters to stop polio epidemics, Greenberg felt that “a scientific examination of the data, and the manner in which the data were manipulated, will reveal that the true effectiveness of the present Salk vaccine is unknown and greatly overrated.” With respect to the field trials of the Salk vaccine before mass vaccination programs were rolled out, he continued, “There were no controls, no rigid diagnostic criteria that could be supervised on a national basis.” He also observed that statistics regarding rates of polio among the unvaccinated were overestimated to the tune of 40% due in part to when a child was considered “vaccinated” (in today’s terms, “fully vaccinated”) because the Salk injected vaccine required multiple shots or boosters and that number changed over time. So a child could have received a polio vaccine injection, but not be considered “vaccinated,” and thus, if stricken with a polio diagnosis, would be counted among unvaccinated children contracting polio.
As you can see, the way a disease is defined is highly important. It determines whether we are in an epidemic and what kind of money a patient, doctor, or hospital gets for treatment. In this age of electronic medical records, algorithms, and artificial intelligence, the diagnosis of a disease also dictates what treatment a patient has access to, reducing the practice of medicine from an art to a formula and increasing patient safety concerns.
Roberts describes a shift in diagnostic criteria from polio to acute flaccid paralysis. Doctors are told to send feces samples to laboratories to test for the presence of a virus and wait to be told if polio was found. These new criteria are influenced largely by the World Health Organization and integrated into CDC guidance for medical practice in the United States.
“This has had the most serious of consequences. One of these is that the power to diagnose polio has been completely taken away from ordinary doctors,” she said “Before 1958, they were taught to diagnose ‘paralytic polio’ as they did other diseases – by observing specific symptoms, particularly acute paralysis and great pain. But doctors are now instructed not to look for the poliovirus itself, as ‘the virus is very hard to find.’ Instead, this task is to be left to WHO and the other governmental agencies that inspect turds. This would be comical if it were not so tragically deceptive.”[12]
Roberts goes on to state that patients previously diagnosed with polio were re-diagnosed under the new rules and a large percentage were found not to have polio.
So, did vaccines eradicate polio? It may depend on how you define polio. In 2018, there was an outbreak of transverse myelitis in California. Some people immediately saw a connection to the feared polio, but the CDC wasn’t calling it that.
“Does the public have any idea that there are hundreds of cases of something that is now called transverse myelitis that would have historically been called polio and is now leaving children permanently dependent on a modern version of the iron lung [called the ventilator]?” –Dissolving Illusions, p. 241.
Statistics have been recorded about how many cases of polio there were when the Salk vaccine was released on the public, but the effect it may have had on what we would call polio is unclear. Might the redefinition of polio changed the numbers? Given these uncertainties, the statistics cannot be seen as reliable at face value, thus we cannot attribute the decline in polio cases to the vaccine.
Further complicating the claim of eradication is the fact that most polio outbreaks at this point are vaccine-strain infections.
TODAY, MOST POLIO FOUND IS VACCINE STRAIN.
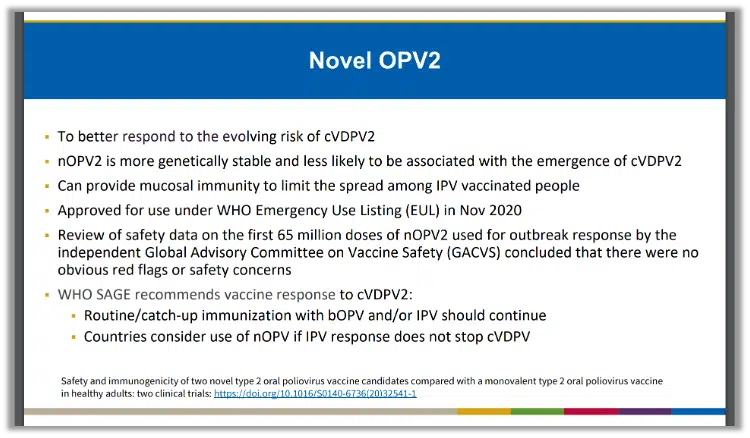
The CDC recently revived a polio workgroup after a case of polio was diagnosed in a New York man in 2022. A patient presented to an ER with fever, neck stiffness, back and abdominal pain, constipation, and muscle weakness, and was diagnosed with polio.[13] If you’ve heard of this case, you’ve probably heard he was “unvaccinated,” but what you might not have heard is the poliovirus that was identified from this man’s stool was vaccine-strain. Below is a slide from a presentation at the October 2022 meeting of the CDC’s Advisory Committee on Immunization Practices (ACIP), confirming the case of polio came from vaccines.

As a result of finding this “cVDPV2,” which means “circulating vaccine-derived poliovirus 2,” the CDC will be beefing up surveillance of polio by sampling wastewater around the country, which can conveniently be done now that an infrastructure was created to monitor COVID in human waste.[14] The Polio Vaccine Workgroup is also monitoring progress on a vaccine to counteract the vaccine-strain polio, with the ultimate goal of recommendation, following WHO guidance. If you’re interested in learning more, a recording of that presentation can be found here (the link will take you right to the slide below in the discussion).
It was reported at ACIP’s February meeting that a vote to recommend adult polio vaccination is anticipated in June 2023. In that same presentation, it was stated there have been no more cases of paralytic polio reported after the New York case was found in 2022, and “most adults in the United States have a low risk of poliovirus exposure and paralytic polio, and most adults received primary polio vaccination series as children.”[15]
CONCLUSION
To bring the journey through polio history full circle, how would you answer the questions posed at the beginning of this article?
Was polio eradicated?
Is it possible?
REFERENCES AND SOURCES
[1] Cueto, M., Brown, T.M., Fee, E.. The World Health Organization, a History. Cambridge University Press. 2019. P. 86.
[2] Bookchin, D., Schumacher J., The Virus and the Vaccine, St. Martin’s Griffin Edition. 2005. (p. 34).
[3] Offit, P. The Cutter Incident. Yale University Press. 2005.
[4] https://www.cdc.gov/vaccinesafety/concerns/concerns-history.html
[5] Read more about Bernice Eddy’s courageous and brilliant work in books like Fear of the Invisible by Janine Roberts, and The Virus and the Vaccine by Debbie Bookchin & Jim Schumacher.
[6] https://www.cnbc.com/2021/07/30/cdc-study-shows-74percent-of-people-infected-in-massachusetts-covid-outbreak-were-fully-vaccinated.html
[7] Cueto, M., Brown, T.M., Fee, E.. The World Health Organization, a History. Cambridge University Press. 2019. P. 63.
[8] https://collections.nlm.nih.gov/ext/dw/101540522/PDF/101540522.pdf (page 10)
[9] Humpries, S., Bystrianyk, R., Dissolving Illusions. 2013. (p. 232); primary source https://archive.org/details/illinoismedicalj1171illi/page/90/mode/2up?q=discussion (pages 85, and 161).
[10] https://archive.org/details/illinoismedicalj1171illi/page/90/mode/2up?q=discussion
[11] Roberts, J. Fear of the Invisible. Impact Investigative Media Productions. 2008 (page 65).
[12] Roberts, J. Fear of the Invisible. Impact Investigative Media Productions. 2008 (page 66).
[13] https://www.cdc.gov/mmwr/volumes/71/wr/mm7144e2.htm
[14] https://www.cdc.gov/nwss/index.html
[15] https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2023-02/slides-02-23/Polio-02-Kidd-508.pdf
Additional Resources
Allen, A. (2007). Vaccine: The controversial story of medicine’s greatest lifesaver. W.W. Norton.
This book does a great job of elucidating the “political use of vaccination” across decades and different diseases, in a journalistic style.
Bookchin, D., & Schumacher, J. (2005). The virus and the vaccine: Contaminated vaccine, deadly cancers, and government neglect. St. Martin’s Griffin.
One of the best books out there to dive deep into SV40–what was known, what was suppressed, and what was at stake.
Cowan, T. D. (2018). Vaccines, autoimmunity, and the changing nature of childhood illness. Chelsea Green Publishing.
This book is written by a doctor who has looked outside the confines of germ theory. One chapter is dedicated to polio and it is a good read to give a quick overview of polio epidemics from the health professional perspective (including effects of pesticides).
Humphries, S., & Bystrianyk, R. (2015). Dissolving illusions: Disease, vaccines and the forgotten history. CreateSpace.
This book should be on the shelf of every health freedom advocate. The chapter on polio is exhaustive, and saturated with citations, If you want to go further into the pesticide side of the polio story, this is your book.
Maready, F. (2018). The moth in The iron lung: A biography of polio. Feels Like Fire.
This book is a “biography of polio” and it looks at the history from a very approachable angle, with lots of storytelling.
Roberts, J. (2009). Fear of the invisible an investigation of viruses and vaccines Hiv and Aids. Impact Investigative Media Productions.
Investigative journalist Janine Roberts did a deep dive into production of vaccines after meeting the family of a child injured by the MMR. Her book is fantastic because it is told first person as she takes you on her journey of uncovering something she never expected–that our vaccines are not as safe as we might believe. There are 2 chapters dedicated to polio including SV40.
Vargha, D. (2021). Polio across the iron curtain: Hungary’s Cold War with an epidemic. CAMBRIDGE UNIV PRESS.
Very rarely do we hear the story of polio and its vaccine outside of the American context. This important history helps us have a bigger picture of the social, economic, and political factors at play globally when it came to the creation of the polio vaccine.