More combos, less choice.
Highlights
- This article is a companion to measles, mumps, and rubella individually.
- Making MMR a combination shot, and removing the availability of the individual measles, mumps, or rubella vaccines, was a policy and profit decision.
- Vaccines have weakened the protection a mother can give naturally and generationally. The very policy aimed at eliminating measles created new vulnerability. By reducing natural infection, widespread vaccination has diminished maternal immunity across generations — leaving infants more susceptible and prompting new calls to vaccinate even earlier. The solution is the problem.
- Dr. Andrew Wakefield dared to call for an investigation between MMR and autism in an oft-cited 1998 Lancet publication and became public health enemy number 1. What do you need to know about “the Wakefield paper” to make an informed decision as a parent?
- A CDC scientist became a whistleblower in 2014, exposing a CDC cover-up of scientific study results showing that African American boys under age 3 had a 340% increased risk of autism after MMR.
- Two formerMerck virologists became whistleblowers in 2010, revealing fraud in studies given to the FDA about mumps vaccine efficacy. The resulting case was resolved in Merck’s favor 14 years later on a technicality.
Choice is taken away from parents by combo shots
If doctors could give your kid one shot with all the vaccines at once, they would. The “simplification” of the vaccine schedule has been the goal since the first meeting of the CDC’s Advisory Committee on Immunization practices (ACIP) in 1964, which launched the childhood vaccine program as we know it. 1

This holy grail of vaccinology has long been a dream, but always an undercurrent. Since the inception of influenza vaccine research a century ago, there have been attempts to create a universal flu vaccine for any strain, and researchers are still trying!2 Most recently, as part of “Generation Gold Standard” under the Trump administration, a new effort has been announced to create a “universal vaccine platform” for multiple pathogens in one. 3
Of course, one shot is less stressful to administer than many. And the more visits needed, the less likely the patient is to receive any shot at all. It should be no surprise that combination shots are created with the specific intent to get more vaccines into more kids; it’s about policy and profits, rather than clinical best practices.
What remains unspoken is the fact that combining shots takes away choice. The classic example is when a person is told in an emergency room they need a tetanus shot for a wound, but not told tetanus is available only in combination with diphtheria and maybe pertussis too. We see the lack of respect for choice expressly stated in a 2006 article in “Drugs of Today” about the development of the combination MMR-V, which combined the MMR shot, which had “almost 100% coverage,” with varicella (chickenpox), which had “significantly lower uptake of 84%.” The author concludes, “The ProQuad combination vaccine facilitates implementation of varicella vaccination into routine childhood immunization schedules and will help protect children against these four potentially serious diseases.” To translate, “facilitates implementation” means it makes it easier to carry out or advance a policy by removing barriers. It’s concerning when the primary factor for changing a nationwide pediatric recommendation is not based on optimal health outcomes, but on administrative logistics.
Combination vaccines have been called the “cornerstone” of vaccine programs, but most research and development is not focused on combination shots.4 Perhaps this is not surprising.Why would a manufacturer focus manpower and money on combining existing shots when there’s a much bigger payoff for creating a new product?
However, despite the “superabundance”5 of the ever-increasing, “saturated” list of recommended shots for our kids and pregnant moms, combination shots are seen as “the future.”6 Why? Because there are even more shots in the pipeline, and the more they add the more resistance, or “barriers to access,” they meet.


In fact, the World Health Organization (WHO) planned its first meeting of its new Technical Advisory Group on Combination Vaccines to run alongside the Global Vaccine and Innovation Research Forum in Rio de Janeiro, Brazil, in March 2025.7 Combo shots are seen as important in advancing the Agenda 2030 and the Sustainable Development Goals.

History of the MMR combo
The 1960s marked a major turning point in vaccine development for two reasons: New technologies for growing viruses in eggs and embryos expanded research possibilities9, and the U.S. government viewed the polio vaccine as a triumph it hoped to replicate.
As explored in Shining a Light on Measles, the drive to develop a measles vaccine was scientific ambition, not a public health crisis. Prominent scientists likened it to conquering Mount Everest — we do because we can. Even leading epidemiologists believed society had adapted to the virus and it was no longer a major threat.
The mumps vaccine was in the same category — the illness considered a nuisance but not a serious threat to children. The military considered mumps a national security threat during WWII, but that market was not big enough. As described by a surgeon of the United States Public Health Service in 1945, “Mumps in civilian populations does not usually constitute a serious public health problem. Epidemics are relatively infrequent, mortality negligible, and disability in children is usually of mild degree with few complications.”
Merck was at the forefront of making these vaccines, and they found themselves in a pickle. They had two vaccines with no market because the illnesses they aimed to prevent were considered common, mild, expected, and generally self-limiting. Nonetheless, U.S. health authorities saw vaccine development as a means of demonstrating scientific leadership. Top scientists at the Public Health Service (the forerunner to the CDC) boasted in an official statement that measles could be eliminated within four years of vaccine introduction.10 That was delayed a few decades, and the World Health Organization launched a global measles eradication initiative through its Expanded Programme on Immunization in the 1970s. Scientific bravado was high — but public demand was not.
But the general populations weren’t concerned with lofty scientific shows of might or what an international organization set its sights on. They had to be convinced to care. So Merck had a costly conundrum. How do you sell a product when there’s no market? What if it’s inescapably bundled with a product the public does want?
Measles was licensed in 1963 and mumps in 1967. (Remember, the mumps vaccine was the fastest developed product before COVID.) These two vaccines were invented and licensed when another common childhood illness was surging, as it did every 6-9 years: rubella. Known as German Measles, rubella wasn’t considered a serious threat for children either. It wasn’t until the 1940s when an ophthalmologist noted a correlation between pediatric cataract patients and their mother’s rubella infections during pregnancy that any concern arose around mumps. However, debate about whether that singular finding was scientifically accurate and significant went on for years.
Licensed in 1969, the rubella vaccine was immediately recommended for all children, in order to protect babies in the womb. The stage was set for quick acceptance by the public with statistics that tens of thousands of babies had been miscarried or born with serious developmental disability during the previous epidemic. The horrors of thalidomide (a drug for morning sickness that caused severe birth defects) were being revealed, with images of deformed children all over the media.
Within two years, Merck was able to hitch the measles vaccine to the rubella vaccine, which did have a market, and add mumps as well. Interest in the rubella vaccine alone waned after the epidemic passed, but the federal government was invested in seeing the measles vaccine succeed, so packaging the three vaccines together was a stroke of sales brilliance for Merck.
The MMR (and Measles-Rubella MR) was licensed in 1971, but interestingly the CDC didn’t officially recommend a mumps shot until 1977. The popular website History.com opines that we wouldn’t have a mumps vaccine if it hadn’t been grouped with measles and rubella.11

The MMR has been around since 1971, but that doesn’t mean it’s been the same all that time. For example, the rubella portion was swapped from Merck’s design to Stanley Plotkin’s RA-27 fetal cell line version after it was determined by researchers the vaccine was safer and more effective when grown on aborted fetal cells, rather than chicken egg cell cultures.
Why isn’t the MMR vaccine given before a child’s first birthday?
The first dose of MMR is recommended for infants between 12 and 15 months. Why not younger? Infants below 12 months old are not given the MMR because their mother’s protection is so effective it stops the vaccine from working.
As one study put it, “Maternal antibodies passed to the fetus during pregnancy impair vaccine efficacy in younger infants.”12 In other words, mothers give their babies antibodies to pathogens through the placenta before birth and in their milk following birth.
The effect isn’t limited to components of the MMR. A publication in the journal “Vaccine” in 2015 noted, “Immune responses to all types of vaccines, including live-attenuated, inactivated, and subunit vaccines, have been reported to be inhibited by the presence of maternal antibody.”13 This raises an important question: If maternal antibodies inhibit the immune response to all vaccine types, why are 29 doses of vaccines administered during infancy on the current schedule?
As it turns out, mothers who were vaccinated against measles instead of having a natural infection have fewer and shorter-lasting antibodies to give to their babies.14 This means MMR recommendations are leaving infants less protected than they would be if nature ran its course. Vaccines have weakened the protection a mother can give naturally and generationally. The very policy aimed at eliminating measles created new vulnerability. By reducing natural infection, widespread vaccination has diminished maternal immunity across generations — leaving infants more susceptible and prompting new calls to vaccinate even earlier. The solution is the problem.

Undetected retroviruses
In 2010, researchers discovered that MMR vaccines had been contaminated with avian retroviruses — specifically, avian leukosis virus (ALV) and endogenous avian retrovirus (EAV). These viruses had gone undetected for decades because older technology couldn’t identify them. According to pro-vaccine outlet Vaxopedia, these contaminants had been present in the vaccine since its creation, we just didn’t have the technology to find it.15
While follow-up studies claimed these retroviruses do not pose a threat to human health16, the fact remains: They were not known to be there. This underscores a critical point for informed consent — vaccine risks are not always identified before widespread use. History has shown that contaminants can go undetected for years, and safety assurances often come after mass administration.17

Mumps vaccine and the U.K. meningitis outbreak
In the early 1990s, the United Kingdom (U.K.) withdrew a dangerous MMR vaccine that caused meningitis 2-4 weeks after the shot, but took four years to do it. After seeing a cluster of meningitis cases after vaccination in the city of Nottingham, England, that “suggested a risk of 1 in 4,000 doses, substantially higher than previous estimates based on case reports from pedaeatricians (4 per million),” the government decided to investigate.18 In a study published in the Lancet, it was assessed the risk was around 1 in 11,000 doses of Urabe-strain mumps vaccine.
The British newspaper “The Independent” reported in 1992 that “children received vaccine despite meningitis risk.”19 It was told that the government spent four years ascertaining whether there was a link, while thousands of children were being vaccinated without parents knowing there was a question about safety. The article doesn’t focus on those four years where parents were not informed of a potentially serious increased risk; it focuses on the days between when the government decided it needed to pull the recommendation for brands with a dangerous strain of mumps vaccine and when they actually told the public. The Independent reported that officials delayed announcing the withdrawal in order to secure enough doses of the alternative MMR II vaccine. Their public health priority was uninterrupted coverage, not transparency.
In 1994, a U.S. Institute of Medicine (IOM) report acknowledged the need for further investigation into whether the Urabe strain of mumps virus caused aseptic meningitis. This reflects a broader pattern in vaccine safety evaluation: Many risks are not definitively studied until after a product is licensed and in widespread use.
The IOM also recommended further study into thimerosal, a mercury-containing preservative found in some vaccines. This foreshadowed future public concern and the subsequent Omnibus Autism Proceedings in U.S. vaccine court, where our federal government summarily dismissed the claims of thousands of families citing vaccine-induced autism in children from either the MMR shot or thimerosal-containing shots – and claims were dismissed after evaluating only a few “test cases.”20 These examples show how the drug industry and specifically the vaccine program has a track record of waiting for postmarket safety evaluations, instead of honoring the precautionary principle, raising serious questions about the depth of informed consent that is possible. Time after time we see safety investigations secretly done after vaccine licensure, while parents are left in the dark about potential risks.
At the same time our federal government was doubling down on vaccine policy with Clinton’s Comprehensive Childhood Immunization Initiative, leading to widespread federal payments of schedule-shots through Vaccines for Children21 and the corollary global push for more, the public was starting to see cracks in the foundation and to ask questions. It was at this moment that Andrew Wakefield and colleagues stepped on to the international stage to highlight big questions that needed to be asked.
What about Wakefield?
You may have heard the name Andy Wakefield. His story has been told many times, including in his own (highly recommended) book “Callous Disregard.” In short, he was falsely accused of writing a paper that said MMR causes autism, causing vaccine hesitancy to skyrocket, shot rates to decline, and epidemics to explode. By honestly reporting what parents told him as a clinician22, he became the face of the government- and industry-scorned “anti-vaccine” movement.

Wakefield was deemed public health enemy number 1! Is it true? Did one man really have the power to change vaccine rates around the globe with one simple publication? Why would he and “that paper” still be a threat today, almost 30 years later? It is certainly possible for one person to make massive change, but there’s more than meets the eye in the public execution of Wakefield’s character and career. He was at the center of a terrible storm where a growing number of doctors and devastated families were finding their own links between autism and vaccines, and governments wanted to destroy that mounting association with no questions asked. Wakefield became their scapegoat. Even before Wakefield came along, the public’s perception of this combination shot had already been shaken by the meningitis link.
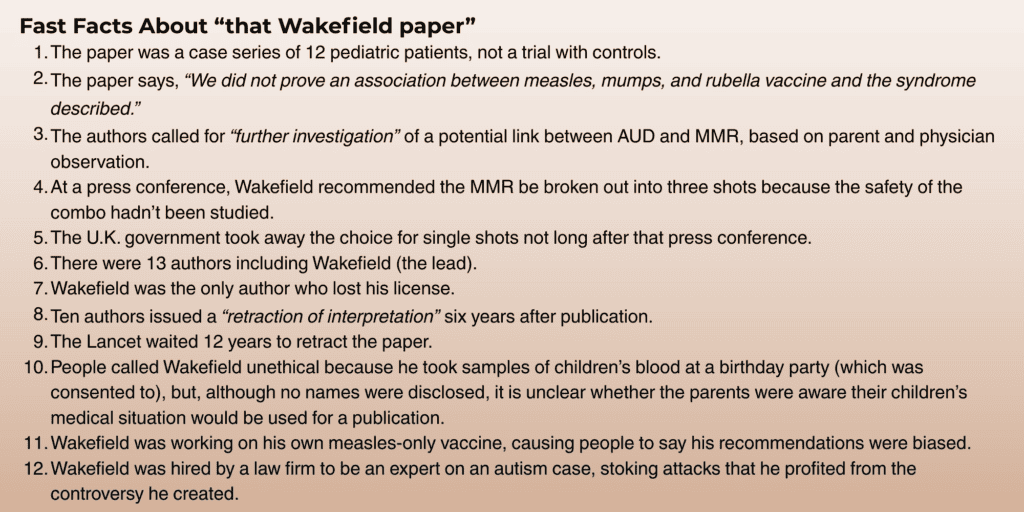
Most people who talk about “that Wakefield paper” haven’t read it, haven’t even seen its title.23 Here it is:

In layman’s terms, this is a report on 12 children who sought treatment for intractable gut issues and developmental disorder without a clear cause. It’s a case series – not a clinical trial. MMR is relevant in the publication as part of the children’s medical history because the parent or physician of 8 of the 12 children linked the onset of behavioral problems with administration of measles, mumps, and rubella vaccination.
In the One Dream interview, Wakefield explains there was debate among the authors about whether to include the MMR connection. He asked, “Why not?” and insisted on reporting the facts as they were given by the parents, respecting their role as parents and caregivers. As revealed in the podcast, the authors debated whether to mention MMR at all, but Wakefield held strong on keeping it in, despite colleagues telling him he was risking his career. He trusted that the medical and scientific community would want honest feedback. So the authors proceeded to share the clinical history of their patients, but perhaps trying to hedge anticipated pushback on questioning the sacred cow that is vaccination, the 13 authors of the paper made it crystal clear in writing they were not saying MMR causes autism. They were not studying the MMR, but a potential link between gut health and autism spectrum disorders in specific children. But they committed the professional sin of noting that information given by parents and doctors needed “further investigation.”

Here is the offending conclusion: “We have identified a chronic enterocolitis in children that may be related to neuropsychiatric dysfunction. In most cases, onset of symptoms was after measles, mumps, and rubella immunisation. Further investigations are needed to examine this syndrome and its possible relation to the vaccine.” (emphasis added)
The study had no controls because it was not an experiment or trial. It was a case study, which is a common type of publication used by practicing doctors to quickly bring attention to a pattern they see in their practice, with the intent that further investigation be done. A press conference was held after the publication and Wakefield did take the position that the MMR should be broken out into three shots because the safety of the combo hadn’t been studied.
The fallout was swift and vicious. But notably, of the 13 authors, only three were investigated for misconduct. One of the investigated, Dr. Murch, was not sanctioned, as GMC noted he was “instrumental in the retraction of the interpretation that had been placed on The Lancet article by the media.” In other words, because Murch orchestrated 11 authors to publicly reject the “interpretation” of their writing, he was left alone. Dr. Walker-Smith initially lost his license, but he appealed and it was reinstated. Wakefield lost his license and abandoned his appeal.
Wakefield was accused of having a financial bias in linking autism and the MMR. He had filed a patent that included a measles-only vaccine and other therapeutics involving the gut illnesses he was researching and attempting to treat in his patients. He says he filed to make sure he protected the financial interests of all involved in the research, even before the product was finalized, and indeed, the patent was never granted nor commercialized.24 Does that mean he had a financial interest that clouded his professional judgment? We can be cynical and say yes, it’s financially better for him if the combo is deemed dangerous. But also, even in a capitalist society, it is plausible that the tail isn’t wagging the dog. If Wakefield thought the triple-shot was dangerous, wouldn’t that be motivation to try to make a better product?
He also received money from the U.K.’s Legal Services Commission as an expert to investigate the safety of the MMR.25 During his hearings with the General Medical Council, he defended his participation in the government-funded investigation with a statement: “If these diseases are found to be linked to the MMR vaccine, these children are the few unfortunate who have been sacrificed to protect the majority.” That was 1997. If the MMR has been dangerous since at least then, how many more children have been seriously injured?

In a striking move, after Wakefield recommended separate shots instead of the combo MMR, the U.K. government took away the choice. In Wakefield’s own words: “In the fall of 1998, six months after The Lancet paper was published, choice in the United Kingdom was denied to parents when the government removed the license for the importation of the single measles vaccine. Let me state that again. At a time when demand for single vaccines was at its highest and parents were choosing to continue vaccinating against measles, mumps, and rubella with the single vaccines, choice was removed. When I asked a senior member of the United Kingdom’s equivalent of the CDC why, she said that allowing parents to choose single vaccines would destroy their established MMR program.
“Nevertheless, removing the choice between the triple vaccine and single vaccines did not have the effect they intended – parents chose not to vaccinate against MMR rather than to use the triple vaccine, and MMR vaccination rates fell in the United Kingdom. The regulators chose to protect policy above children.”26 So was the drop in MMR rates a result of a publication or an unpopular policy?
Here’s your TLDR summary: Did MMR rates fall after the “Wakefield paper” was released? Yes. Did MMR rates fall because Wakefield said MMR causes autism? No. There were other forces at work, including parental instinct and oppressive government policy. Did Wakefield do anything at all that a critical mind could question? Of course; he’s human. Did he deserve to become public health enemy number 1? No.
We encourage you to read the whole sordid story in his own words in his book “Callous Disregard.”27
What does the CDC know about the MMR-autism link?
Americans have been told ad nauseum and with a religious-type fervor that vaccines don’t cause autism. What is that based on? According to current Secretary of Health and Human Services (HHS) Robert F. Kennedy, Jr., three of the main studies the CDC relies upon by their own scientists were published in 2004, 2007, and 2010. Dr. William Thompson, who was a senior scientist at the immunization office, was author or coauthor on all three studies.28 Thompson spoke to scientific researcher and father Dr. Brian Hooker, in 2002-2004 when Hooker tried to advise on CDC vaccine safety studies for neurodevelopmental disorders, but was stopped when Hooker filed a petition for vaccine injury for his son with autism in the vaccine court. Thompson reached out again in 2013-2014 to help Hooker access data that had been hidden and examine the science. Thompson was able to deliver potentially classified information to Hooker in a legal way by educating him on the “citizen’s request.”
Thompson revealed that the CDC manipulated autism-vaccine-link studies, and “omitted statistically significant information” that showed African American boys who got the MMR before the age of 3 were at a 340% higher risk of autism than those who delayed the shot. The Institute of Medicine (IOM) used studies that Thompson worked on to “slam the door on future autism and vaccine research.”29 Thompson was ready to “stop lying.” He regretted playing a part in a fraud that put autism research 10 years behind because the CDC was not transparent. (It’s now been 20 years.)
Unbeknownst to Thompson, Hooker recorded four of their calls and made them public. Read “Vaccine Whistleblower” by Kevin Barry, Esq. for a full transcript. Thompson did not deny his statements, instead becoming a whistleblower, funneling copies of hidden CDC data to Congressman Bill Posey.
Watch Congressman Posey bring the information to Congress and call for an investigation on July 29, 2015. He reads a quote from Thompson who describes a meeting with coworkers and superiors where researchers were ordered to put their research in a garbage can, but Thompson did not.
The Orlando Sentinel reported that Posey had been quietly working with families for years, who believed their child’s autism was linked to vaccines.30 When Thompson approached him with documents to back up his claims, Posey took a stand on the floor of Congress, calling on colleagues to do their jobs to exercise oversight over the accused executive agency. Just like our current HHS Secretary Kennedy, he was called many names, but nobody answered the questions.

As reported in “Vaccine Whistleblower,” “In the 2007 study, CDC scientists removed the low IQ individuals with autism or other neurological diagnosis from the pool before even beginning their study on Thimerosal exposure.”31 This was at the same time the U.S. Senate investigation led by senator and practicing physician Tom Coburn found “widespread corruption and mismanagement at the CDC’s vaccine programs.”32 A year later, an investigation by HHS found “97% of special government advisors on committee in the CDC vaccine program failed to disclose necessary information about conflicts of interest,” which led to criminal investigations.33
According to the book, “Thompson now confesses that he and his fellow CDC researchers found a strong autism signal in children who received the MMR vaccine before their third birthday. Then, under orders from their bosses and in violation of the study protocols, the scientists eliminated this data from the final published study, in order to fool the public about vaccine safety.”34

Conclusion
The government’s decision to eliminate access to individual measles, mumps, and rubella vaccines in favor of the combined MMR shot was not made with families in mind. It exemplifies the worst kind of one-size-fits-all, government-backed medicine — where bureaucratic convenience and pharmaceutical interests trump parental concerns, scientific transparency, and individualized care.
The stories of Dr. Andrew Wakefield and CDC whistleblower Dr. William Thompson illustrate the high cost of questioning this system. Wakefield’s call for further investigation — not a definitive claim — was met not with inquiry, but with professional ruin. Thompson, meanwhile, revealed that critical data suggesting a heightened risk of autism in certain populations following the MMR vaccine was concealed, not debated.
These are not anomalies; they are symptoms of a larger culture that suppresses dissent, buries risk, and refuses to adapt — even as the childhood schedule grows more bloated and trust continues to erode.
As Wakefield wrote:
“When you are stonewalled or these answers are not to your satisfaction, trust your instinct. I say this as someone who has studied and engaged in the science and who has become aware of the limitations of our knowledge and understanding of vaccine safety issues. Maternal instinct, in contrast, has been a steady hand upon the tiller of evolution; we would not be here without it.”
— Andy Wakefield, The Suppression of Science, Vaccine Epidemic, 2011
This is not just a scientific issue — it’s a human rights issue. As Wakefield affirmed:
“In the spirit of the Constitution, the people will have their say — vaccination choice is a human right.”
— The Suppression of Science, Vaccine Epidemic, 2011
The future of health freedom depends on our willingness to question authority, demand transparency, and defend the right of every family to make informed medical decisions — especially when government and industry refuse to do so.
References:
- “Minutes, Meeting No. 1, Advisory Committee on Immunization Practices, May 25-26, 1964.” CDC Stacks, (1964). https://stacks.cdc.gov/view/cdc/77545. ↩︎
- Nachbagauer, Raffael, and Peter Palese. “Is a Universal Influenza Virus Vaccine Possible?” Annual Review of Medicine 71, (2020): 315-327. https://pubmed.ncbi.nlm.nih.gov/31600454/. ↩︎
- HHS, NIH Launch Next-Generation Universal Vaccine Platform for Pandemic-Prone Viruses.” HHS Press Office, (2025). https://www.hhs.gov/press-room/hhs-nih-announces-generation-gold-standard.html. ↩︎
- Oberman, Elayna. “Fewer Shots, More Protection: The Promise of Combination Vaccines.” PATH, (2025). https://www.path.org/our-impact/articles/fewer-shots-more-protection-the-promise-of-combination-vaccines/#:~:text=Furthermore%2C%20this%20week%20on%20the%20sidelines%20of,on%20the%20strategic%20development%20of%20this%20work. ↩︎
- Hausdorff, William P. PhD, et al. “Facilitating the Development of Urgently Required Combination Vaccines.” The Lancet 12, no. 6 (2024). https://www.thelancet.com/journals/langlo/article/PIIS2214-109X(24)00092-5/fulltext. ↩︎
- “Combination Vaccines Could Be the Future of Immunization Programs.” PATH, (2024). https://www.path.org/our-impact/articles/combination-vaccines-could-be-the-future-of-immunization-programs/. ↩︎
- Oberman, Elayna. “Fewer Shots, More Protection: The Promise of Combination Vaccines.” PATH, (2025). https://www.path.org/our-impact/articles/fewer-shots-more-protection-the-promise-of-combination-vaccines/#:~:text=Furthermore%2C%20this%20week%20on%20the%20sidelines%20of,on%20the%20strategic%20development%20of%20this%20work. ↩︎
- “Terms of Reference for the Technical Advisory Group on Combination Vaccines.” World Health Organization, (2020). https://cdn.who.int/media/docs/default-source/immunization/product-and-delivery-research/tors-combos-final.pdf?sfvrsn=d0a92ec0_1. ↩︎
- Roos, Dave. “How a New Vaccine Was Developed in Record Time in the 1960s.” History, (2020). https://www.history.com/articles/mumps-vaccine-world-war-ii. ↩︎
- Sencer, David J. MD, H. Bruce Dull MD, and Alexander D. Langmuir MD. “Epidemiologic Basis for Eradication of Measles in 1967.” Public Health Reports 82, no. 3 (1967). https://pmc.ncbi.nlm.nih.gov/articles/PMC1919891/pdf/pubhealthreporig00027-0069.pdf. ↩︎
- Roos, Dave. “How a New Vaccine Was Developed in Record Time in the 1960s.” History, (2020). https://www.history.com/articles/mumps-vaccine-world-war-ii. ↩︎
- Anonymous. 2002. Turtles All the Way Down: Vaccine Science and Myth. Edited by Zoey O’Toole, and Mary Holland J.D., p.358. https://www.amazon.com/Turtles-All-Way-Down-Vaccine/dp/9655981045. ↩︎
- Edwards, Kathryn M. “Maternal Antibodies and Infant Immune Responses to Vaccines.” Vaccine 33, no. 47 (2015): 6469-6472. https://www.sciencedirect.com/science/article/pii/S0264410X15010634#:~:text=of%20vaccine%20responses-,Infants%20are%20born%20with%20immature%20immune%20systems%2C%20making%20it%20difficult,exclusion%20and%20neutralization%20%5B3%5D. ↩︎
- Edwards, Kathryn M. “Maternal Antibodies and Infant Immune Responses to Vaccines.” Vaccine 33, no. 47 (2015): 6469-6472. https://www.sciencedirect.com/science/article/pii/S0264410X15010634#:~:text=of%20vaccine%20responses-,Infants%20are%20born%20with%20immature%20immune%20systems%2C%20making%20it%20difficult,exclusion%20and%20neutralization%20%5B3%5D. ↩︎
- Iannelli, Vincent MD. “Are Vaccines Contaminated with Retroviruses?” Vaxopedia, (2018). https://vaxopedia.org/2018/12/29/are-vaccines-contaminated-with-retroviruses/. ↩︎
- Khan, Arifa S. PhD. “Investigating Viruses in Cells Used to Make Vaccines; and Evaluating the Potential Threat Posed by Transmission of Viruses to Humans.” FDA Science & Research (Biologics), (2024). https://www.fda.gov/vaccines-blood-biologics/science-research-biologics/investigating-viruses-cells-used-make-vaccines-and-evaluating-potential-threat-posed-transmission. Tsang, Shirley X. et al. “Evidence of Avian Leukosis Virus Subgroup E and Endogenous Avian Virus in Measles and Mumps Vaccines Derived from Chicken Cells: Investigation of Transmission to Vaccine Recipients.” Journal of Virology, (1999). https://pmc.ncbi.nlm.nih.gov/articles/PMC112645/pdf/jv005843.pdf. ↩︎
- Victoria, Joseph G. et al. “Viral Nucleic Acids in Live-Attenuated Vaccines: Detection of Minority Variants and an Adventitious Virus.” Journal of Virology 84, no. 12 (2010). https://journals.asm.org/doi/10.1128/jvi.02690-09. ;
Hussain, A I. et al. “Lack of Evidence of Endogenous Avian Leukosis Virus and Endogenous Avian Retrovirus Transmission to Measles, Mumps, and Rubella Vaccine Recipients.” Emerging Infectious Diseases 7, no. 1 (1999): 66-72. https://pmc.ncbi.nlm.nih.gov/articles/PMC2631681/. ↩︎ - Miller, E. MFPHM, et al. “Risk of Aseptic Meningitis after Measles, Mumps,and Rubella Vaccine in UK Children.” The Lancet 341, no. 8851 (1993): p 979-982. https://www.thelancet.com/journals/lancet/article/PII0140-6736(93)91069-X/fulltext. ↩︎
- https://www.independent.co.uk/news/uk/children-received-vaccine-despite-meningitis-link-1551697.html ↩︎
- Omnibus Autism Proceeding.” U.S. Court of Federal Claims,. https://www.uscfc.uscourts.gov/omnibus-autism-proceeding. ↩︎
- “Celebrating 30 Years of Vaccines for Children (VFC).” David J. Sencer CDC Museum,. https://www.cdc.gov/museum/online/vfc.html. ↩︎
- “WAKEFIELD EPISODE TITLE.” One Dream Podcast with Dr.Nick and Leah Wilson. Video, https://podcasts.apple.com/us/podcast/one-dream-podcast-with-dr-nick-and-leah-wilson/id1443439682. ↩︎
- Wakefield, A J. et al. “Ileal-lymphoid-nodular Hyperplasia, Non-specific Colitis, and Pervasive Developmental Disorder in Children.” The Lancet 351, (1998): p.637-641. https://www.thelancet.com/pdfs/journals/lancet/PIIS0140-6736(97)11096-0.pdf. ↩︎
- “Day 31 GMC Fitness to Practice Hearing for Andrew Wakefield.” Wakefield GMC Transcripts, (2012). https://wakefieldgmctranscripts.blogspot.com/2012/02/gmc-fitness-to-practice-hearing-for.html?utm_source=chatgpt.com. ↩︎
- Dyer, Owen. “Wakefield Tells GMC He Was Motivated by Concern for Autistic Children.” British Medical Journal 336, no. 7647 (2008): 738. https://pmc.ncbi.nlm.nih.gov/articles/PMC2287213/?utm_source=chatgpt.com. ↩︎
- Habakus, Louise K., Mary Holland M.A., J.D, and Kim M. Rosenberg J.D. 2012. Vaccine Epidemic: How Corporate Greed, Biased Science, and Coercive Government Threaten Our Human Rights, Our Health, and Our Children. Skyhorse. p. 232. https://www.amazon.com/Vaccine-Epidemic-Corporate-Coercive-Government/dp/1620872129., ↩︎
- Wakefield, Andrew J. 2017. Callous Disregard: Autism and Vaccines — The Truth Behind a Tragedy. Skyhorse. https://www.amazon.com/Callous-Disregard-Autism-Vaccines-Tragedy/dp/1510729666. ↩︎
- Wakefield, Andrew J. 2017. Callous Disregard: Autism and Vaccines — The Truth Behind a Tragedy. Skyhorse. https://www.amazon.com/Callous-Disregard-Autism-Vaccines-Tragedy/dp/1510729666. ↩︎
- Barry, Kevin. 2017. Vaccine Whistleblower: Exposing Autism Research Fraud at the CDC. Skyhorse. https://www.amazon.com/Vaccine-Whistleblower-Exposing-Autism-Research/dp/1510727302, page xxi. ↩︎
- Powers, Scott. “Rep Posey at Center of Vaccine-Autism Fight.” Orlando Sentinal https://www.orlandosentinel.com/2015/08/21/rep-posey-at-center-of-vaccine-autism-fight/. ↩︎
- Barry, Kevin. 2017. Vaccine Whistleblower: Exposing Autism Research Fraud at the CDC. Skyhorse. https://www.amazon.com/Vaccine-Whistleblower-Exposing-Autism-Research/dp/1510727302, page xv. ↩︎
- Barry, Kevin. 2017. Vaccine Whistleblower: Exposing Autism Research Fraud at the CDC. Skyhorse. https://www.amazon.com/Vaccine-Whistleblower-Exposing-Autism-Research/dp/1510727302, page xvii.; Coburn, Tom M.D. . “CDC Off Center.” The U.S. Senate Subcommittee on Federal Financial Management, (2007). https://coburn.library.okstate.edu/coburn/pdf/cdc_off_center.pdf. ↩︎
- Barry, Kevin. 2017. Vaccine Whistleblower: Exposing Autism Research Fraud at the CDC. Skyhorse. https://www.amazon.com/Vaccine-Whistleblower-Exposing-Autism-Research/dp/1510727302, page xvii. ↩︎
- Barry, Kevin. 2017. Vaccine Whistleblower: Exposing Autism Research Fraud at the CDC. Skyhorse. https://www.amazon.com/Vaccine-Whistleblower-Exposing-Autism-Research/dp/1510727302, page xiv, foreword by Robert F, Kennedy Jr. ↩︎