The STD vaccine that exploited cancer fears
This is Part 1 of a two-part series. In this article we will learn what HPV is and how big a threat. We’ll look at the creation of the vaccine and its effect on cervical cancer rates.
In Part 2, we’ll dive into the marketing machine behind the shot, the safety risks, and the governmental actions supporting the shot.
Highlights
- HPV is a sexually transmitted disease that clears on its own most of the time.
- There’s no herd immunity argument for the HPV vaccine. A person can’t catch it simply by standing next to someone who has it.
- The CDC tells us “HPV infections are very common. Nearly everyone will get HPV at some point in their lives.”
- In contrast, cervical cancer, which is supposedly caused by HPV, is very rare in the U.S.
- Evidence suggests that the HPV shot may cause the cancer it claims to prevent.
- The time that experts recommend getting the HPV shot is a policy decision, not a medical decision. The vaccine is suggested for 11–12-year-olds to increase vaccine uptake by giving the shot when children would be in the office for other recommended shots.
- The HPV shot story gives us another reason to be concerned about School-based Health Centers, which offer the medical establishment a way to push the HPV vaccine. Schools have been a proven route for increasing HPV shots overall — without parental consent in some states.
Introduction
The more you know, the less you fear. And when fear is in the driver’s seat, our minds and hearts are not. That’s why we’re going to tell you the story of the HPV vaccine, which is advertised to prevent cancer, so you can make an informed decision about this heavily promoted shot.
The National Cancer Institute tells us that cervical cancer is very rare in the U.S., making up only 0.7% of new cancer cases in the country.1 By their count, it is 20th on the list of the most common cancers.

So why do we need a shot for our kids, marketed as the “cervical cancer vaccine,” for a cancer that is very rare? Are the risks of the shot worth the benefit advertised?
The HPV vaccine story takes a lot of twists and turns, winding down many paths. This article will give you a map so you know where to start your research if you want to explore further. Although HPV is associated with multiple cancers, this article will address cervical cancer, as that’s the focus of the vaccine’s promotion.
Let’s dive into the story of how Gardasil was added to the U.S. childhood immunization schedule.
What is HPV?
HPV stands for human papillomavirus. A papilloma is “a benign (noncancerous) tumor arising from an epithelial (skin or mucus membrane) surface and usually known to grow in an outward direction.”2 Basically, they’re warts.3 They occur on animals as well as humans (hence the name human papillomavirus). Papillomaviruses “ramp up normal growth functions” in cells.4 HPV is generally not considered dangerous, often having no symptoms at all. Most, if not all, sexually active people encounter HPV.
HPV is a sexually transmitted disease. Itt’s usually transferred skin-to-skin and via mucous membranes, but one scientific publication reports, “HPV is very resistant to heat and desiccation (drying out), and nonsexual transmission via [contaminated surfaces] can also occur, such as by prolonged exposure to shared contaminated clothing.”5 That type of transfer is much less likely, but still exists. As with tetanus, there’s no herd immunity argument for the HPV vaccine. A person can’t catch it simply by standing next to someone who has it.
Interestingly, it is also very rare for a mother to pass HPV to her child during birth and, in those rare cases, the infection clears itself quickly.6

There are over 240 types of HPV identified in animals and humans.7 “At least 14 are classified as high-risk HPV types, known as HPV 16, 18, 31, 33, 35, 39, 45, 51, 52, 58, 59, 66, and 68,” and associated with cancers.8 The rest are referred to as low risk. HPV is associated with many types of growths, benign or cancerous. The virus group has been linked to cervical, vulvar, penile, anal, mouth, and throat cancers.9
Most types of HPV are not associated with cancer. In other words, having an HPV infection does not mean cancer is inevitable. In fact, you’d be hard pressed to find a major public health association that doesn’t agree that 90% of HPV infections clear themselves, with no lasting effects.

As an aside, don’t confuse HPV with HSV, herpes simplex virus, though it’s easy to do. In fact, before the discovery of HPV, it was wondered if herpes virus caused cervical cancer.10 Both viruses are sexually transmitted, affect the skin, and cause growths.11 In general, HPV is associated with warts and cancer while herpes is associated with ulcers and blisters and can alternate between flare-ups and dormant stages. Only two types of herpes have been identified, causing either cold sores around the mouth or genital blisters, but there are hundreds of types of HPV.
How is HPV associated with cervical cancer?
HPV isn’t a direct cause of cervical cancer. Instead, it’s associated with abnormal cervical cell growth, and that is considered a potential precursor to cancer. HPV was linked to cancer in the 1980s when strains were found in cervical cancer cell samples.
The CDC tells us “HPV infections are very common. Nearly everyone will get HPV at some point in their lives”12 (emphasis in original). They tell us that nine out of ten cases will resolve themselves within two years, and most people don’t know they have it.13 It is so common that a person can be infected with multiple types at once.14 However, we know that it’s not universal for women to be diagnosed with cervical cancer. What makes the difference if HPV is said to cause cervical cancer?
Something we don’t hear about often: It’s estimated that 3-15% of cervical cancers worldwide are HPV-negative.15 A 2022 study revealed that “cervical cancer cases that are HPV-independent are being reported steadily in clinical practice.”16 Researchers do believe there are false-negatives, but still “truly non-HPV” cases do exist and need to be studied more.
It wasn’t until the dawn of polymerase chain reaction (PCR) technique in the late 1980s that the scientific community fully embraced HPV as the cause of cervical cancer.17 (You may have heard of PCR most recently associated with COVID tests.) Before PCR was created, there was debate over whether HPV caused cervical cancer, if another virus was involved, or none at all. PCR was used to target what researchers saw in cancerous cells and multiply it to a large enough quantity so they could tell what it was. Scientists decided that HPV causes cancer because they detected certain strains in cancerous cells.

But HPV doesn’t directly cause cancer. Something happens between having a detectable amount of HPV in the body and having a cervical cancer diagnosis. This is where the waters get muddy.
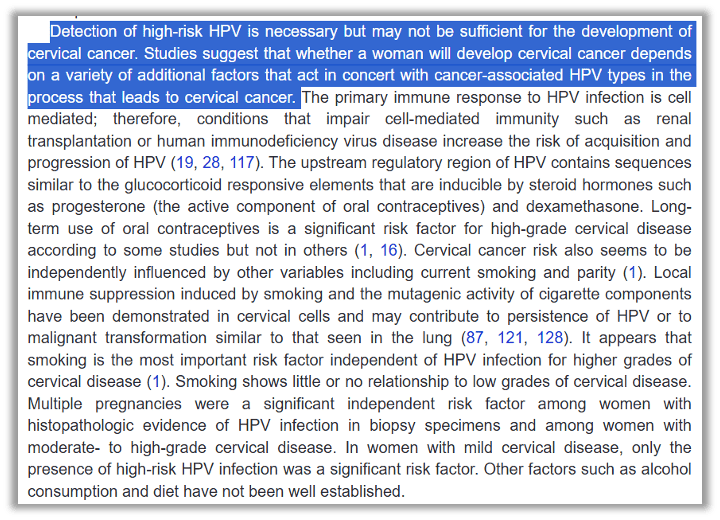
Here’s a way to think about it: HPV can be found in most, if not all, people once they become sexually active. Some of those sexually active women are diagnosed with abnormal cells on the cervix, and only some womenwith abnormal cells get cervical cancer.

The abnormal cells are known by different names: “cervical dysplasia,” “cervical lesions,” or “cervical intraepithelial neoplasia,” (CIN). The severity is assessed as mild “1,” medium “2,” or severe “3.” This grading system was introduced in 1973 to promote the concept of a disease continuum from precursor lesions to invasive cancer”18 (emphasis added). In other words, the grades were made up to promote the idea that a person first gets HPV, then has abnormal cells that get continually worse, (level 1, 2, then 3) and eventually turn into cancer. This might be helpful for a medical coder, but reality doesn’t fit into the nice boxes medicine is trying to force it into.
Between the almost universal experience of HPV infection and the very rare situation of cervical cancer, those abnormal cells will come and go. The abnormal cells will go away on their own most of the time. In 2007, the New England Journal of Medicine published an editorial that explained the Grade 2 abnormality “is not an irrefutable cancer” predictor and, therefore, “current guidelines suggest that some young women with such lesions do not need to be treated” at all.19
According to one gynecologic oncologist at University of Texas MD Anderson Cancer Center:20

Given the fact that cervical cancer can exist without the detection of HPV, one might wonder about the validity of the assertion that HPV is the cause of cancer. Perhaps it’s simply present while cancer is too. But without that direct-line-thinking from HVP to cervical cancer, one might say there is no market for an HPV vaccine.
In short, there is no direct line from HPV infection to cancer, most HPV infections will not end in a cancer diagnosis, and it is possible to have cervical cancer without HPV present.
Cervical cancer is slow growing. The World Health Organization states it takes 15-20 years after HPV infection for cervical cancer to appear.21
The logical flip side to the coin of consensus that 90% of people’s HPV infections go away on their own, is that 10% do not. The CDC tells us on their website that about 10% of women with HPV infections will develop cancer.22 Unfortunately, the CDC does not cite any source for this, so it leaves one wondering if they mean any woman, anywhere, or just in the U.S.?
It’s a well-understood fact that cervical cancer is much more prevalent in low-income countries that do not have access to pap smears. That statistic also makes one wonder what happened to the other types of cancer associated with HPV — if 90% of HPV cases clear on their own, and 10% of cases turn into cervical cancer, how many are getting anal, throat, or other cancers? There’s no percentage left!
The CDC estimates there are an average of 11,500 new cases of cervical cancer each year in the U.S., with 4,000 deaths.23 Those cases and deaths are generally associated with poverty, which affects access to regular care.24 About 80% of cervical cancer is diagnosed in the developing world.25 This is because in resource-rich countries like the U.S., “threat of disease is blunted by rigorous screening practices.” And cervical cancer death rates in the U.S. dropped 72% between 1955 and 1992 — years before the HPV vaccine was created.
Are there other ways to prevent or cure HPV or cervical cancer?
According to the FDA and the CDC, there’s no cure for HPV, but there are treatments for the health problems they believe it causes.


However, a research team in Mexico is credited with discovering a cure for HPV using photodynamic therapy.

The only reporting from major news outlets on this phenomenal discovery was an attempt to debunk the doctor’s research because it hadn’t yet been published in a peer-reviewed journal. And they made sure to remind everyone to get the vax. But even Snopes couldn’t deny this one, stamping it with a green check mark and declaring it true.26 Though Dr. Eva Ramón Gallegos faced many years of marginalization as a female doctor in Mexico tackling the target of a blockbuster drug, her research was published in 201727 and again in 2023 in Photochemical Photobiology.28
More to ponder on your risk/benefit analysis of the HPV vaccine
Being aware of known risk factors for HPV infection and cervical cancer, as well as prevention techniques or treatments empowers you to make informed choices.
- Abstinence from any sexual contact prevents HPV infection.
- Fewer sexual partners (and with people who have also had few) lessens the chances of HPV infections.
- Monogamous relationships do not allow for foreign HPV.
- Screening for abnormal cells or HPV presence has been known to prevent cervical cancers or allow for the earliest possible treatment.
- Carrageenan, a carbohydrate found in red seaweed and commonly used as a food additive, has been found to inhibit HPV. 29
- Photodynamic therapy has been used to eliminate HPV.
- Smoking is associated with a higher likelihood of cervical cancer.
- Multiple pregnancies are associated with a higher likelihood of cervical cancer.
Is there any natural immunity for HPV?
Published research shows us natural immunity exists, though researchers claim they do not know how long it lasts.30 Researchers in 2016 found “significant protection against subsequent infection.”31 Another research team in 2021 found natural immunity to be “highly protective,” calling for further studies, notably because it was “crucial to determine the extent of HPV natural immunity to accurately model the effectiveness of different vaccination strategies.”32 Without knowing who is already immune to HPV, it’s impossible to untangle whether a decline in HPV happens naturally or because of a vaccine.
Notably, a 2009 study found natural immunity protects against more than one strain.33 The authors made hopeful comments that the quadrivalent (four-strain) vaccine would also protect against more than those four strains. But they also pointed out that may not be the case because the vaccine uses “virus-like particles” rather than the whole virus as it is contracted naturally.
How was the vaccine developed?
In 1983 and 1984, a team of scientists led by Harald zur Hausen was credited with isolating HPV-16 and HPV-18 and hypothesizing the strains led to cervical cancer.34 He and his team used the new technology of polymerase chain reaction, known as PCR, to increase the DNA found in the cell samples for study.35 Zur Hausen was awarded the 2008 Nobel Prize for Medicine for this achievement. Shockingly, zur Hausen reported that his attempts to engage the pharmaceutical industry for vaccine development failed because it was believed there was no market for it.

Using PCR as an identification tool was the first technological advance needed to pave the way for the vaccine.36 The second technological breakthrough was the ability to genetically modify viruses.37
The HPV vaccine was tremendously difficult to make.38 Four teams around the globe were at the forefront of research: the National Cancer Institute, the University of Rochester, Georgetown University, and Queensland University in Australia. Each team, working independently but simultaneously, contributed to the body of work that became HPV vaccines.
If you’re wondering why four separate teams would put tremendous effort into creating a vaccine without a market, you can look at it altruistically as cervical cancer is a top killer of women in developing countries. But perhaps a more practical reason is that the value of the market (once created) was estimated in the billions. In fact, there was a 13-year-long battle over royalties between all the players listed above, which ended only when Merck and GlaxoSmithKline agreed to pay royalties to everyone. As the authors of “The HPV Vaccine on Trial” put it, “Fame, fortune, and the sheer joy of discovery were at stake.”39
Generally, viruses are isolated, and then researchers must be able to grow them in a lab to have enough material to work with. The HPV virus did not grow easily. After attempts with human warts, cow warts, and fragments of cervixes failed, University of Rochester researchers turned to human foreskin from circumcisions.40 Foreskins were infected with genital warts, then attached to mice bred specifically to be unable to reject foreign tissue.41 This technique “eventually provided enough virus for continued research.”42
Replicating whole virus was one step, but to create a vaccine, scientists need something that, in theory, won’t cause the illness they’re trying to prevent. Typically, viruses would be weakened (“attenuated”), but that wasn’t working for HPV. Ultimately, scientists figured out how to recreate the shell, so to speak, of the HPV, without the DNA inside. This was known as a “virus-like particle,” or VLP. Eventually, researchers at the University of Queensland in Australia, as well as NIH, genetically modified the virus into VLPs, and each filed patents on their findings.43 A team at Georgetown University in Washington, D.C., also filed a patent around the same time for work on HPV proteins. Shortly thereafter, a patent was filed by the Rochester researcher for his virus isolation techniques. All these techniques led to the creation of the HPV vaccines by Merck in the U.S. and GlaxoSmithKline in the U.K.
At Merck, the team was led by Dr. Kathrin Jansen, who would later join Pfizer and lead COVID shot development. The Merck team built on the work done by the four research groups and took a gamble on creating an HPV vaccine in the 1990s when there was still doubt that HPV caused cervical cancer. The Merck clinical trials are claimed to have laid those doubts to rest.44

What is efficacy?
What is the HPV vaccine supposed to be able to do? Direct-to-consumer advertising has done a good job of blurring the line between HPV and cervical cancer, so many people may quickly say, “Gardasil prevents cancer.”
The drug was initially marketed as a cervical cancer vaccine, and is still referred to as such by health professionals, including the Director of HPV Vaccination Programs for the Bill & Melinda Gates Foundation.45 The Gardasil label claims the vaccine will “help protect individuals ages 9 to 45 against” illnesses caused by nine strains of HPV, including cervical, vulvar, anal, vaginal, throat, and mouth cancers, as well as genital warts. Gardasil 9 includes strains 6, 11, 16, 18, 31, 33, 45, 52, 58.

As you can see, Gardasil claims to do a lot. Messaging in more recent years has started highlighting the other claims of Gardasil. A quick browser search with predictive text shows us people have a lot of questions about what exactly this shot is meant to do.

For each one of those illnesses Gardasil claims to protect against, a different efficacy is reported, which also varies by age group.46
Note that “efficacy” and “effectiveness” are not the same thing when it comes to pharmaceuticals. Here’s how Gavi (a global vaccine alliance) describes it:

Efficacy is imaginary. It’s how much researchers estimate a vaccine will “prevent disease, and possibly also transmission, under ideal and controlled circumstances.”47 It’s what scientists strive for in a lab — the best possible hope for what their product could do. On the other hand, in the real world, we see how effective a vaccine is when used by various age groups, who have underlying conditions, and use other medications. simultaneously. Also contributing to the shot’s effectiveness: the possibility of different strains, how the vaccine is stored and administered, and a host of other complicating factors. These real-world complications take that ideal, imaginary number of efficacy down to reality.
Effectiveness is measured by observation once the vaccine is licensed. In other words, no one knows how well (if at all) a vaccine will work until it’s unleashed on the public, but we know for sure it won’t perform as well as it did in controlled trials. That’s true for all drugs the FDA gives it’s thumbs up to, not just Emergency Use Authorized products. Gavi assures us, however, that “Vaccines do not always need to have an exceptionally high effectiveness to be useful.”
With respect to claims about preventing cervical cancer, things get a little complicated. The FDA did not require Merck to show it prevented cervical cancer. Instead, it allowed Merck to use a different “endpoint” to declare their product a success. Remember that the medical world wants us to think of the path to cervical cancer as linear steps down a road directly from HPV to increasingly serious abnormal cells on the cervix and ending at cervical cancer. Assuming this was correct, the FDA allowed Merck to use the Grade 2 or 3 abnormal cells as the “endpoint” to claim success.48 This decision prompted days of discussion by its Vaccines and Related Biologics Product Advisory Committee (VRBPAC), with a number of people questioning its appropriateness.49 Ultimately, Merck was graced with the FDA’s go-ahead. This was very important for Merck because GlaxoSmithKline had a rival product, Cervarix, and Merck wanted the American market.
Peter McCullough published an article on July 30, 2024, on his Substack summarizing a recent study from the Journal of the American Medical Association (JAMA) analyzing 14 years of effectiveness data for the HPV vaccine.50 The news isn’t good. He reports that the data show the vaccine fails to prevent “precancerous” Grade 2 and 3 abnormal cells.
Could the HPV shot cause the cancer it claims to prevent?
It’s commonly understood among health professionals that the vaccine doesn’t work if a person has already been infected (in other words, is sexually active or has suffered sexual abuse). The Cleveland Clinic states on their website, “If you’ve already been exposed, the vaccine won’t provide much benefit.”51 “The Women’s Health Activist” published in 2007, “The vaccine only works if it is administered before a woman is exposed to HPV.”52 Merck itself admits the vaccine won’t work if a person has already been exposed or, of course, if they are exposed to a strain not in the shot.53

The CDC warns us as well:

Regardless, the American College of Obstetricians and Gynecologists (ACOG) recommends HPV shots after exposure anyway, reasoning a person probably hasn’t been exposed to all nine strains in the current vaccine.54 In the case that a person is vaccinated after infection, the efficacy rate drops. One recent study reviewed effectiveness studies from 2007-2022 and saw a range of effectiveness from 12%-90% for the age range of 15–18-year-olds.55 One of the studies reviewed illustrates the quick drop in efficacy as a child approaches 18 from 89.1% to 28.9%.

But things might be more serious than simply having an ineffective vaccine. Does the shot cause the thing it’s claiming to prevent? In “The HPV Vaccine on Trial,” the authors tell us, “Shortly after FDA approved the vaccine, [Dr. Sin] Lee contacted the FDA to make the case that girls must be tested for HPV infection before getting the vaccine. He believed that there was a real risk that the vaccine itself might trigger a dangerous reaction in HPV-infected girls and women that could accelerate abnormal cervical cell growth.”56 He based that belief on data from the trials. The book also reveals that “in the trials, Merck reported that women who had a current HPV 16 or 18 infection and evidence of prior exposure to those types on Day 1 were 44.6 percent more likely to develop CIN2 or CIN3 lesions or worse compared to the fauxcebo [fake placebo] group, even within a few years of receiving the vaccine.”57 The authors go on to observe that women who had current or past infections have “negative efficacy” of -33.7%, meaning not only did the shot not work to prevent infection, people who got the shot were almost 34% more likely to get cancer.
Dr. Lee was able to test 16 sealed vials of Gardasil from around the world and found that every one of them contained HPV DNA contamination.58 When he contacted the FDA, he was told they were already aware of the “DNA fragments,” but the vaccine was still “safe and effective.” This was surprising because the vaccine was supposed to contain no DNA, only the virus-like particle, which was the outer shell without the DNA inside.
It leaves one to wonder, why are the CDC and the FDA and every medical professional pushing this shot without recommending the very simple HPV DNA screening test first? In fact, ACOG recommends young women through the age of 26 get the shots, “regardless of sexual activity, prior exposure to HPV, or sexual orientation, if they were not vaccinated in the target age of 11-12 years.”59
This is the reason the HPV shot is given to young children: because younger kids are less likely to have been exposed to HPV through sexual encounters. It’s also noteworthy that the CDC recommends this shot for people in prison60 and some states require the shot for foster children.61 Both of these groups have often already been exposed to HPV.
Further, it has been noted that women who believe they’re getting a “cervical cancer vaccine” think they can stop getting regular screenings, assuming they won’t get cancer because they got the shots. Thus any potential cervical cell changes go undetected making them more likely to become cancer, which won’t be found until it’s much further along.
In August 2024, researcher Jen Margulis published an analysis of the data we have for cervical cancer since the rollout of the vaccine.62 In short, the kids who were vaccinated around the age of 12 are adults now, and we’re seeing a rise in cervical cancer among that age group.

An article published on PLOS ONE (the first multidisciplinary peer-reviewed journal to focus on rigorous research and ethics rather than perceived impact) in July 2024 asserted the same failure of the vaccine, though in more conservative terms.63 It said, “It is interesting to see that since the introduction of the vaccines, incidence and mortality rates of cervical cancer have remained relatively stable nationally.” In other words, the vaccine has had no effect on reducing rates.

So we have this absurd and outrageous state of affairs where policymakers are pushing a pharmaceutical product on children to reduce cancer, but the ultimate outcome might be more cancer.
Ever-expanding CDC recommendations
The CDC’s Advisory Committee on Immunization Practices (ACIP) announced in June 2024 the resurrection of a working group for the HPV vaccine. They want to address the push by “stakeholders” to give the vaccine at age 9, to provide more “guidance” for the “shared clinical decision-making” for those aged 27-45 who want the shot, and to evaluate whether one dose would suffice.64
Here’s the evolution of HPV vaccine recommendations, per the ACIP.
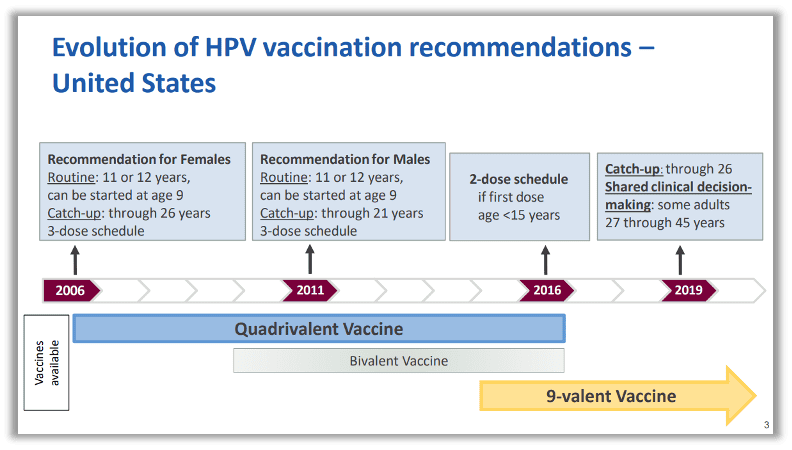
The timing of this work group also aligns with Merck’s recent announcement that they are evaluating whether one shot is enough, as opposed to the two or three shots currently recommended.65 Merck will also begin recruiting for a new trial to test adding more strains of HPV to their cocktail, with a focus on types more prevalent in people of African or Asian descent.
Why consider different wording for kids as young as age 9? Could it be a new recommendation?And why did the ACIP choose to recommend the shot for 11–12-year-olds, rather than 9-year-olds, for whom the shot has been approved? The hope was to increase vaccine uptake by bundling the shot with another time children would be in the office for other recommended shots, namely meningococcal, Tdap, and yearly influenza. They wanted to build up the “adolescent vaccine platform.”66
Make no mistake about it: The time that experts recommend getting the HPV shot is a policy decision, not a medical decision.

The lens of policy applies even if we’re thinking of how young the shot is given. These recommendations are one-size-fits-all. HPV is a sexually transmitted disease, and sexual choices are highly personal, individual, and value-based. This is the same policy logic as giving all babies hepatitis B vaccines, which were created for a virus that is transmitted via risky behavior such as sexual activity and needle use (or medical mistakes). The government’s justification for subjecting all children to the same recommendation is, basically, “you never know” which child will go down the path of high-risk behaviors.
And that ACIP endorsement is gold. As reported in PharmExec.com: “[E]ven Merck insiders admit that it was ACIP’s coverage recommendation that really put things in motion. Within five months of ACIP’s decision, and by the time Merck launched its big consumer push, CDC had added Gardasil to its Vaccines for Children contract, providing it free of charge to uninsured girls ages 9 to 18. Most states took up the cause by establishing cervical cancer task forces, and all but one pledged to cover the prophylactic vaccine. The private sector followed their lead, with 95 percent of plans adding Gardasil to their formularies.” This is the power of the childhood schedule. It doesn’t have to be law; it’s driven by money and influence.
Unfortunately, the bundling backfired, and providers got feedback that parents wanted fewer shots at once, not more. Bundling was a barrier to acceptance. So stakeholders want the ACIP to use stronger words, which will hopefully trigger more doctors recommending the shot at younger ages, ultimately lead to more shots in arms.
But let’s back up a little. Why is the HPV shot, a vaccine for sexually transmitted diseases, recommended for kids as young as age 9? There are two strong reasons. The first was discussed above: The shot doesn’t work if a person has already been exposed to the strain. So policymakers want to vaccinate as young as possible to minimize giving the shot to those who have had sexual contact. The second reason is that no one wants to talk to kids about sex.

Both parents and doctors would prefer to avoid the topic of sexual activity with children.67 One of the benefits cited for giving the vaccine to children as young as 9 years old is to reduce the stigma around the thought of a child being sexually active. (And not just any child, but your child). Further, giving the shot at a young age will quiet those who believe that giving the vaccine will cause sexual promiscuity, since the child is so young. It is a supremely immature and irresponsible policy, but that’s what it is.
Merck zeroed in on something they could get parents — and more importantly their kids — talking about: fear about the potential for cancer decades later. This brings us full circle to why the shot was marketed as a “cervical cancer vaccine,” rather than what it is: an STD vaccine.
School-based Health Centers and minor consent
The next battleground for informed consent is the School-based Health Center (SBHC). “School-based vaccine education, outreach, and delivery are key strategies recommended by the World Health Organization to introduce the HPV vaccine into national vaccine programs.”68
School-based medical care has been eyed up for many years as a way to push the HPV shot in particular. It’s the shot on the childhood schedule with the lowest percentage of uptake before COVID. And schools have been a proven route for increasing HPV shots overall.69

Stand for Health Freedom has been at the forefront of monitoring the rapidly expanding use of School-based Health Centers in the United States. These centers are much more than a school nurse’s office. They are meant to be a “medical home” for our children, offering primary care and any other type of medical service a school chooses to include. The Biden administration has been pouring hundreds of millions of dollars into making grants available for schools to create and grow SBHC’s.70 This administration’s focus has been on mental health and “reproductive care” (which casts a long shadow in terms of what services can be included).71 HPV vaccines are considered reproductive care.72
A big danger associated with SBHC’s is that many states have lowered the age of consent for medical and/or reproductive care. Further, state privacy laws prevent parents from being able to access records of what is being diagnosed, treated, or prescribed at SBHCs for their own children, because records belong to the provider and laws protect the patient, no matter what age.

Websites like “Vaxteen” counsel kids on trying to get around parental consent laws by pointing them to Title-X clinics where they can get “some health care services without parental consent” including vaccinations.
Merck, the maker of Gardasil, is a primary funder of the national School Based Health Alliance (SBHA).73 They funded the creation of the SBHA’s “Toolkit To Increase Well-Child Visits And Vaccinations In School-Aged Youth.”74 For context, Merck makes 11 of the 14 vaccines on the CDC’s recommended childhood schedule, (three have no competitors — HPV, MMRV, and chickenpox) so they have a lot to gain by promoting vaccine administration in schools outside of parental presence.75
Conclusion
The HPV vaccine story is deep and complex, and this article can only skim the surface. We urge you to look deeply into this shot and the risks associated with it. Stay tuned for Part 2 of this story, where we will look at manipulative marketing tactics, along with very serious safety concerns for the shot.
To Learn More
- SHF handout titled HPV facts at a glance.
- “The Greater Good” documentary
- “Sacrificial Virgins” documentary
- “The HPV Vaccine on Trial” book
- Interviews with people involved with “The HPV Vaccine on Trial”
- Article discussing problematic clinical trials
- “Gardasil: Fast-Tracked and Flawed” book
References
- “Cancer Stat Facts: Cervical Cancer.” National Cancer Institute, (2024). https://seer.cancer.gov/statfacts/html/cervix.html. ↩︎
- Sabry, Ahmed O., and Bhupendra C. Patel. “Papilloma.” National Library of Medicine, StatPearls, (2023). https://www.ncbi.nlm.nih.gov/books/NBK560737/#:~:text=A%20papilloma%20is%20a%20benign%20(non%2Dcancerous)%20tumor%20arising,the%20body%20with%20squamous%20epithelium:. ↩︎
- MacGill, Markus. “Should I Worry about a Papilloma?” Medical News Today, (2018). https://www.medicalnewstoday.com/articles/312657#:~:text=Papillomas%20are%20benign%20growths.,when%20they%20reach%20the%20skin ↩︎
- Goodsell, David. “Molecule of the Month: Human Papillomavirus and Vaccines.” PDB-101, (2018). https://pdb101.rcsb.org/motm/221. ↩︎
- Burd, Eileen M. “Human Papillomavirus and Cervical Cancer.” Clinical Microbiology Reviews, (2003). https://journals.asm.org/doi/10.1128/cmr.16.1.1-17.2003. ↩︎
- Soucheray, Stephanie. “Study: HPV Does Not Often Transmit to Babies during Pregnancy.” CIDRAP, (2023). https://www.cidrap.umn.edu/human-papillomavirus-hpv/study-hpv-does-not-often-transmit-babies-during-pregnancy. ↩︎
- Van Doorslaer, Koenraad. “Evolution of the Papillomaviridae.” Virology 445, no. 1-2 (2013): 11-20. https://www.sciencedirect.com/science/article/pii/S0042682213002924#:~:text=Papillomaviruses%20co-evolved%20with%20their%20hosts.%20%E2%80%A2%20Papillomaviruses%20gained,evolve%205%E2%80%9310%20times%20faster%20than%20their%20mammalian%20hosts. ↩︎
- Yuan, Haobo, et.al. “Phylogenetic Analysis and Antigenic Epitope Prediction for E6 and E7 of Alpha-papillomavirus 9 in Taizhou, China.” BMC Genomics, (2024). https://bmcgenomics.biomedcentral.com/articles/10.1186/s12864-024-10411-1. ↩︎
- “Cancers Linked with HPV.” American Cancer Society, https://www.cancer.org/cancer/risk-prevention/hpv/hpv-and-cancer-info.html#:~:text=be%20noticed%20early.-,Anal%20cancer,(mouth)%20and%20throat%20cancers. ↩︎
- “Brand of the Year.” Pharmaceutical Executive, (2007). https://www.pharmexec.com/view/brand-year-0. ↩︎
- “HPV and Herpes: What’s the Difference?” Lloyd’s Pharmacy Online Doctor, https://onlinedoctor.lloydspharmacy.com/uk/sexual-health-advice/hpv-vs-herp ↩︎
- “About HPV.” CDC. https://www.cdc.gov/hpv/about/. ↩︎
- “Basic Information about HPV and Cancer.” CDC, https://www.cdc.gov/cancer/hpv/basic-information.html. ↩︎
- Burd, Eileen M. “Human Papillomavirus and Cervical Cancer.” Clinical Microbiology Reviews, (2003). https://journals.asm.org/doi/10.1128/cmr.16.1.1-17.2003. ↩︎
- Lee, Jae-Eun, et al. “Untold Story of Human Cervical Cancers: HPV-negative Cervical Cancer.” BMB Reports Online, (2022): 429–438. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9537028/. ↩︎
- Lee, Jae-Eun, et al. “Untold Story of Human Cervical Cancers: HPV-negative Cervical Cancer.” BMB Reports Online, (2022): 429–438. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9537028/. ↩︎
- Young, L S, et al. “The Polymerase Chain Reaction: A New Epidemiological Tool for Investigating Cervical Human Papillomavirus Infection.” BMJ 298, (1989). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1835377/pdf/bmj00213-0018.pdf ↩︎
- Burd, Eileen M. “Human Papillomavirus and Cervical Cancer.” Clinical Microbiology Reviews, (2003). https://journals.asm.org/doi/10.1128/cmr.16.1.1-17.2003 ↩︎
- Sawaya, George F. MD, and Karen Smith-McCune M.D., Ph.D. “HPV Vaccination — More Answers, More Questions.” New England Journal of Medicine 356, no. 19 (2007). https://www.nejm.org/doi/full/10.1056/NEJMe078060. ↩︎
- Watson, Sara K. “For Women over 30, There May Be a Better Choice than the Pap Smear.” NPR, (2018). https://ihpi.umich.edu/news/women-over-30-there-may-be-better-choice-pap-smear. ↩︎
- “Human Papillomavirus and Cancer.” World Health Organization, (2024). https://www.who.int/news-room/fact-sheets/detail/human-papilloma-virus-and-cancer#:~:text=It%20usually%20takes%2015%E2%80%9320,a%20foul%2Dsmelling%20vaginal%20discharge. ↩︎
- “Basic Information about HPV and Cancer.” CDC, (2023). https://www.cdc.gov/cancer/hpv/basic-information.html. ↩︎
- [1] “Cervical Cancer Statistics.” CDC, (2024). https://www.cdc.gov/cervical-cancer/statistics/index.html#:~:text=Each%20year%20in%20the%20United,women%20die%20of%20this%20cancer. ↩︎
- Azadnajafabad, Sina, et al. “Health Disparities in Cervical Cancer: Estimating Geographic Variations of Disease Burden and Association with Key Socioeconomic and Demographic Factors in the US.” PLOS ONE, (2024). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11257296/. ↩︎
- “Brand of the Year.” Pharmaceutical Executive, (2007). https://www.pharmexec.com/view/brand-year-0. ↩︎
- Garcia, Arturo. “Did a Mexican Researcher Develop a Potential Treatment for HPV?” Snopes, (2019). https://www.snopes.com/fact-check/eva-ramon-gallegos-hpv/. ↩︎
- Alvarado, Elizabeth M, et al. “Effectiveness of Photodynamic Therapy in Elimination of HPV-16 and HPV-18 Associated with CIN I in Mexican Women.” Photochem Photobiol., (2017). https://pubmed.ncbi.nlm.nih.gov/28380684/. ↩︎
- López-Cárdenas , María T. “Elimination of Human Papillomavirus and Cervical Pathological Microbiota with Photodynamic Therapy in Women from Mexico City with Cervical Intraepithelial Neoplasia I.” Photochem Photobiol., (2023). https://pubmed.ncbi.nlm.nih.gov/36773299/. ↩︎
- Buck, Christopher B, et al. “Carrageenan Is a Potent Inhibitor of Papillomavirus Infection.” PLOS Pathogens, (2006). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1500806/.;
Calagna, Gloria, et al. “‘Secondary Prevention’ against Female HPV Infection: Literature Review of the Role of Carrageenan.” Expert Rev Anti Infect Ther, (2020). https://pubmed.ncbi.nlm.nih.gov/32552158/. ↩︎ - Tian, Tian, et al. “Potential Role of Naturally Acquired Immunity against HPV in the Control of HPV Related Diseases.” Lancet Reg Health West Pac, (2021). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8342770/#:~:text=The%20natural%20immunity%20is%20highly,infection%20should%20be%20further%20studied. ↩︎
- Beachler, Daniel C. “Natural Acquired Immunity Against Subsequent Genital Human Papillomavirus Infection: A Systematic Review and Meta-analysis.” The Journal of Infectious Diseases, (2016). https://pubmed.ncbi.nlm.nih.gov/26690341/#:~:text=67%2D1.77%20%5BP=%20.,HPV%20infection%20in%20female%20subjects. ↩︎
- Tian, Tian, et al. “Potential Role of Naturally Acquired Immunity against HPV in the Control of HPV Related Diseases.” Lancet Reg Health West Pac, (2021). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8342770/#:~:text=The%20natural%20immunity%20is%20highly,infection%20should%20be%20further%20studied. ↩︎
- Malik, Zainab A, et al. “Persistent Antibodies to HPV Virus-Like Particles Following Natural Infection Are Protective Against Subsequent Cervicovaginal Infection with Related and Unrelated HPV.” Viral Immunology, (2009). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2883483/#:~:text=It%20has%20been%20reported%20that,similar%20protection%20is%20not%20known. ↩︎
- “Harald Zur Hausen Biographical.” The Nobel Prize, (2007). https://www.nobelprize.org/prizes/medicine/2008/hausen/biographical/. ↩︎
- Young, L S, et al. “The Polymerase Chain Reaction: A New Epidemiological Tool for Investigating Cervical Human Papillomavirus Infection.” BMJ 298, (1989). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1835377/pdf/bmj00213-0018.pdf. ↩︎
- Andersson, Jan. “The Discoveries of Human Papilloma Viruses that Cause Cervical Cancer and of Human Immunodeficiency Virus.” Nobelforsamlingen at Karolinska Institutet. https://www.nobelprize.org/uploads/2018/06/advanced-medicineprize2008.pdf. ↩︎
- Frazer, Ian H. “The HPV Vaccine Story.” ACS Pharmacology & Translational Science, (2019). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7089001/. ↩︎
- Bryan, Janine T, et al. “Prevention of Cervical Cancer: Journey to Develop the First Human Papillomavirus Virus-like Particle Vaccine and the Next Generation Vaccine.” Current Opinion in Chemical Biology, no. 32 (2016): 34–47. https://sci-hub.st/10.1016/j.cbpa.2016.03.001. ↩︎
- Holland, Mary JD, et al. 2018. The HPV Vaccine On Trial: Seeking Justice For A Generation Betrayed. Skyhorse. page 20. ↩︎
- Bonnez, William, et al. “Isolation and Propagation of Human Papillomavirus Type 16 in Human Xenografts Implanted in the Severe Combined Immunodeficiency Mouse.” Journal of Virology 72, no. 6 (1999). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC110112/. ↩︎
- Mcneil, D. G. (2006, August 29). How a vaccine search ended in triumph. The New York Times. https://www.nytimes.com/2006/08/29/health/29hpv.html. ↩︎
- Holland, Mary JD, et al. 2018. The HPV Vaccine On Trial: Seeking Justice For A Generation Betrayed. Skyhorse. page 21. ↩︎
- “GARDASIL® – the HPV Vaccine: Case Study.” Australia National Health and Medical Research Council, (2023). https://www.nhmrc.gov.au/about-us/resources/impact-case-studies/gardasilr-hpv-vaccine#:~:text=To%20study%20these%20genes%20and,could%20protect%20against%20HPV%20infection. ↩︎
- Scolnick, Edward M. “A Vaccine to Prevent Cervical Cancer: Academic and Industrial Collaboration and a Lasker Award.” Clinical and Translational Immunology, (2017). ↩︎
- Ndiaye, Cathy. “This Cervical Cancer Vaccine Can Prevent Cancer. But More Adolescent Girls Need Access to It.” The Bill & Melinda Gates Foundation, (2025). https://www.gatesfoundation.org/ideas/articles/hpv-vaccine-access-to-prevent-cervical-cancer-senegal. ↩︎
- “Efficacy of GARDASIL 9.” Merck Vaccines. https://www.merckvaccines.com/gardasil9/efficacy/. ↩︎
- Joi, Priya. “What Is the Difference between Efficacy and Effectiveness?” Gavi: VaccinesWork, (2020). https://www.gavi.org/vaccineswork/what-difference-between-efficacy-and-effectiveness. ↩︎
- Holland, Mary JD, et al. 2018. The HPV Vaccine On Trial: Seeking Justice For A Generation Betrayed. Skyhorse. page 45. ↩︎
- VRBPAC Transcript November 28, 2001. https://wayback.archive-it.org/7993/20170404095222/https://www.fda.gov/ohrms/dockets/ac/01/transcripts/3805t1_01.pdf. ↩︎
- McCullough, Peter A. MD, MPH. “Gardasil Fails to Protect Against Cervical Intraepithelial Neoplasia Over Time.” Courageous Discourse, (2024). https://petermcculloughmd.substack.com/p/gardasil-fails-to-protect-against?publication_id=1119676&post_id=147029787&isFreemail=true&r=rgolm&triedRedirect=true. ↩︎
- “HPV Vaccine.” Cleveland Clinic,. https://my.clevelandclinic.org/health/treatments/21613-hpv-vaccine. ↩︎
- Redmond, Malika A. “A Critical Discourse Analysis of the Marketing of Merck & Co.’s Human Papillomavirus Vaccine Gardasil®.” ScholarWorks at Georgia State University, (2011). https://scholarworks.gsu.edu/cgi/viewcontent.cgi?article=1028&context=wsi_theses. ↩︎
- “Indication for GARDASIL 9.” Merck Vaccines,. https://www.merckvaccines.com/gardasil9/?cid=PPC-accountype:MICROSOFT-campaign:Gardasil+HCP_Branded_BRND_NA_HPV+Vaccine_General_EDUC_PHRS_MULTI_2023. ↩︎
- Deak, Pamela MD. “What I Tell Every Patient About the HPV Vaccine.” American College of Obstetricians and Gynecologists, (2020). https://www.acog.org/womens-health/experts-and-stories/the-latest/what-i-tell-every-patient-about-the-hpv-vaccine. ↩︎
- Ellingson, Mallory K, et al. “Human Papillomavirus Vaccine Effectiveness by Age at Vaccination: A Systematic Review.” Human Vaccines & Immunotherapeutics, (2023). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10399474/. ↩︎
- Holland, Mary JD, et al. 2018. The HPV Vaccine On Trial: Seeking Justice For A Generation Betrayed. Skyhorse. page 215. ↩︎
- Holland, Mary JD, et al. 2018. The HPV Vaccine On Trial: Seeking Justice For A Generation Betrayed. Skyhorse. page 68. ↩︎
- Holland, Mary JD, et al. 2018. The HPV Vaccine On Trial: Seeking Justice For A Generation Betrayed. Skyhorse. page 216.
Also: Lee, Sin H. “Detection of Human Papillomavirus (HPV) L1 Gene DNA Possibly Bound to Particulate Aluminum Adjuvant in the HPV Vaccine Gardasil.” Journal of Inorganic Biochemistry, (2012). https://pubmed.ncbi.nlm.nih.gov/23078778/. ↩︎ - “Human Papillomavirus Vaccination.” American College of Obstetricians and Gynecologists, (2020). https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2020/08/human-papillomavirus-vaccination. ↩︎
- “Sexually Transmitted Infections Treatment Guidelines: Persons in Correctional Facilities.” CDC, (2020). https://www.cdc.gov/std/treatment-guidelines/correctional.htm#:~:text=Persons%20are%20likely%20to%20engage,(see%20Primary%20Prevention%20Methods). ↩︎
- “HPV VACCINATION: A Look at State Policy and a Path Forward.” St. Jude Children’s Research Hospital, (2021). https://sjr-redesign.stjude.org/content/dam/research-redesign/centers-initiatives/hpv-cancer-prevention-program/hpv-cancer-prevention-program.pdf. ↩︎
- Margulis, Jennifer. “They Said This Vaccine Would Protect Us Against Cancer. They Lied.” Vibrant Life, (2024). https://jennifermargulis.substack.com/p/they-said-this-vaccine-would-protect. ↩︎
- Castellano, Tara, et al. “Health Disparities in Cervical Cancer: Estimating Geographic Variations of Disease Burden and Association with Key Socioeconomic and Demographic Factors in the US.” PLOS ONE, (2024). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11257296/. ↩︎
- Brooks, Oliver MD. “Introduction to the HPV Vaccines Work Group.” CDC, (2024). https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2024-06-26-28/01-HPV-brooks-508.pdf. ↩︎
- “Merck Announces Plans to Conduct Clinical Trials of a Novel Investigational Multi-Valent Human Papillomavirus (HPV) Vaccine and Single-Dose Regimen for GARDASIL®9.” Merck, (2024). https://www.merck.com/news/merck-announces-plans-to-conduct-clinical-trials-of-a-novel-investigational-multi-valent-human-papillomavirus-hpv-vaccine-and-single-dose-regimen-for-gardasil-9/. ↩︎
- Kaplan, David W. MD, MPH. “Barriers and Potential Solutions to Increasing Immunization Rates in Adolescents.” Journal of Adolescent Health, (2010). https://www.jahonline.org/article/S1054-139X(09)00657-0/abstract. ↩︎
- “Provider Education Series Videos.” American Cancer Society National HPV Vaccination Roundtable, (2023). https://hpvroundtable.org/provider-education-series-videos/. ↩︎
- Shin, Michelle B, et al. “Multilevel Perspectives on School-based Opportunities to Improve HPV Vaccination among Medically Underserved Adolescents: Beyond School Entry Mandates.” Human Vaccines & Immunotherapeutics, (2023). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10478734/. ↩︎
- Shin, Michelle B, et al. “Multilevel Perspectives on School-based Opportunities to Improve HPV Vaccination among Medically Underserved Adolescents: Beyond School Entry Mandates.” Human Vaccines & Immunotherapeutics, (2023). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10478734/. ↩︎
- “Biden-Harris Administration Announces Nearly $100 Million in Continued Support for Mental Health and Student Wellness Through Bipartisan Safer Communities Act.” U.S. Dept of Education, (2023). https://www.ed.gov/news/press-releases/today-biden-harris-administration-announcing-more-95-million-awards-across-35-states-increase-access-school-based-mental-health-services-and-strengthen-pipeline-mental-health-professionals-high-needs-school-districts-t. ↩︎
- “President Biden Highlights Several Important Sexual and Reproductive Health Priorities in His FY25 Budget Request.” (2024). https://www.siecus.org/president-biden-highlights-fy25-budget/. ↩︎
- Santa Maria, Diane, et al. “Nurses on the Front Lines: Improving Adolescent Sexual and Reproductive Health Across Health Care Settings.” The American Journal of Nursing, (2017). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5513155/. ↩︎
- “Our Funders and Partners.” School-based Health Alliance. https://www.sbh4all.org/about/funders-and-partners/. ↩︎
- “Toolkit to Increase Well-Child Visits and Vaccinations in School-Aged Youth.” School-based Health Alliance. https://tools.sbh4all.org/merck-toolkit/merck-toolkit-home/. ↩︎
- “Current CDC Vaccine Price List.” CDC Vaccines for Children Program, (2024). https://www.cdc.gov/vaccines-for-children/php/awardees/current-cdc-vaccine-price-list.html. ↩︎