October 25, 2024
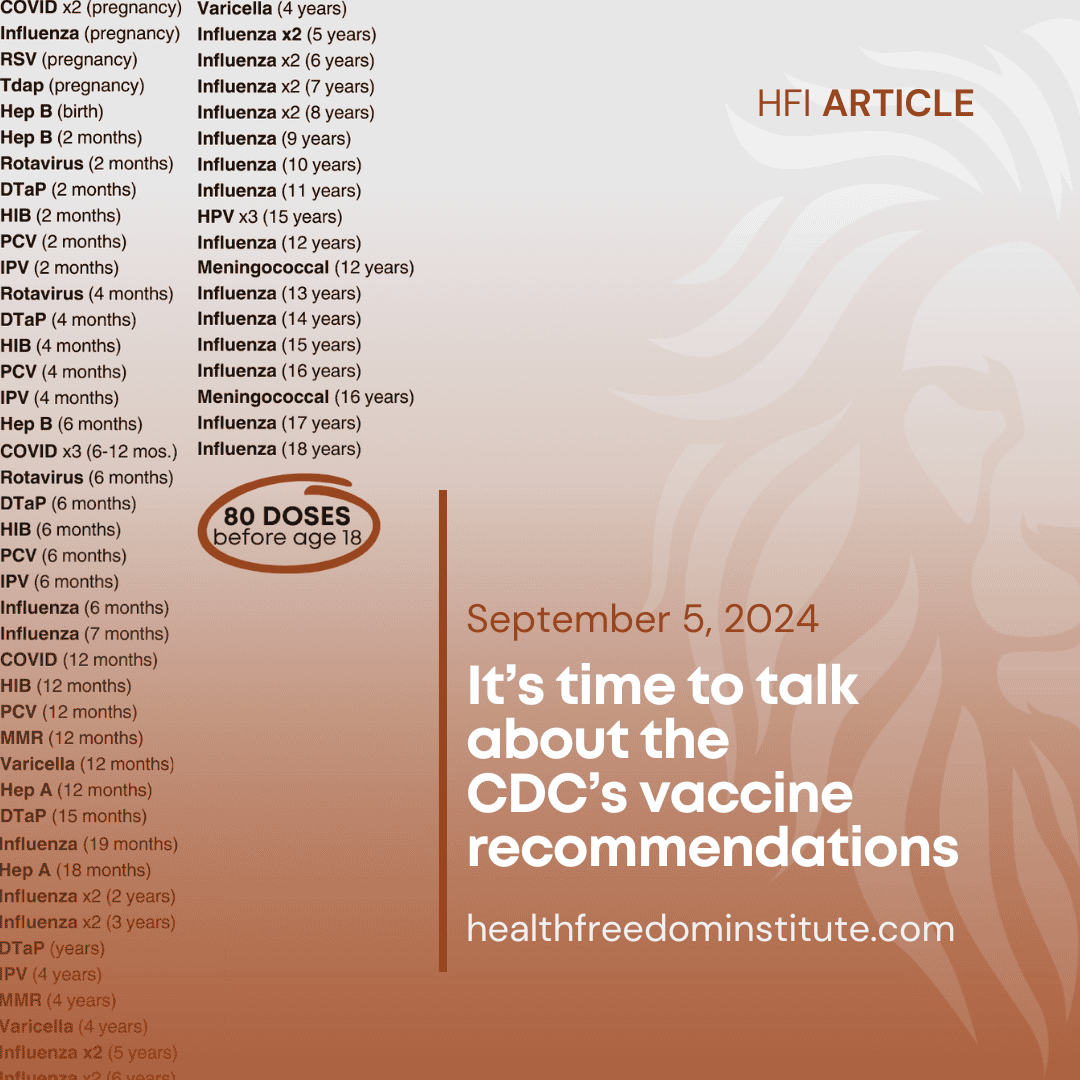
The CDC’s Advisory Committee on Immunization Practices (ACIP) met October 23-24, 2024, for their annual meeting to approve updates to the immunization schedules and discuss other matters. Overall, discussions revolved around how to increase vaccine uptake, with an eye toward adding to the childhood and adult schedules and perhaps creating a new pregnancy schedule.
We’ve chosen the following highlights from the many topics discussed over the two-day meeting.
Summary of votes: (all votes unanimous except pneumococcal)
- A second COVID shot is recommended for people over 65 and for those with moderate to severely compromised immunity.
- The recommendation for the adult pneumococcal vaccine was lowered from age 65 to age 50.
- An additional meningococcal shot was recommended for high-risk kids age 10 and above and suggested for adolescents 16-23.
- The new meningococcal B vaccine was added to VFC (triggers federal purchases).
- Added high-dose and “adjuvanted inactivated” flu vaccines to the VFC for 18-year-olds who have certain organ transplants.
- Approved updates to the childhood and adult immunization schedules.
Discussion themes — all of which pointed back to increasing vaccine uptake
- Recommending vaccines universally based on age, rather than only for those with specific risk factors, increases uptake overall.
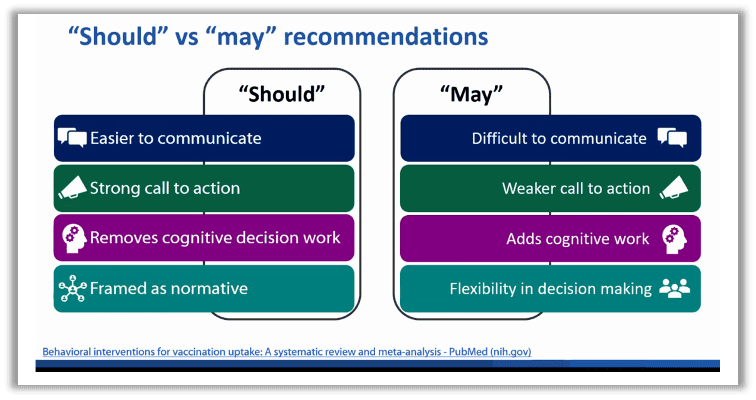
- Telling people they “shall” get a shot is better than saying they “may.” The language ACIP uses is “recommend” vs. “shared clinical decision making.”
- People are more likely to get a vaccine if they’re already in the office for another one.
- Expect more shots recommended during pregnancy.
Note that these themes are about the policy of increasing vaccine sales and use, regardless of what is right for an individual. In fact, what’s right for an individual is abandoned in favor of the policy aims. For example, the ACIP wanted more people at high risk for pneumococcal illness to get the vaccines. So instead of suggesting a public relations campaign to target audiences or educating doctors to reach out to certain patients, the ACIP concluded that making a universal recommendation will increase the chances of all people getting the shot, which, they reason, would include the target group. It doesn’t matter if those who are not at high risk would not get a shot recommendation otherwise. It also doesn’t take into account any specific reasons the minority group may have for not getting the shot. To target a minority population, the ACIP casts a big net and hopes they catch the fish they’re seeking.
Will there be a pregnancy schedule?
While a potential pregnancy schedule was not on the agenda as its own topic, it came up in more than one question and comment, with one commenter saying that a schedule would be necessary because the recommendations are “only going to get more complex as more vaccines come online.”
(HFI’s “Shining a light on meningitis” noted that a Group B streptococcus (GBS) vaccine is on the horizon.) Notably, pregnancy is listed as a “medical condition” in the childhood schedule. This speaks volumes to the medicalization of completely natural human processes. For comparison, sometimes we trip while going down stairs and break a bone, but that doesn’t mean using stairs is a medical condition.
“Should” ACIP give us choices?
There’s been lot of talk at ACIP meetings in the last year or two about using “should” versus “may” in recommendations. One ACIP member noted one of the reasons the word “may,” also referred to as “shared clinical decision making,” is frowned upon by the ACIP is because many vaccines are now given at pharmacies, especially COVID. “Clinical decision making,” a medical analysis with individual advice about the risks and benefits of a shot, isn’t typically in the scope of practice of a pharmacist. What does that mean? If the CDC suggests a doctor and patient have a discussion about whether a vaccine is right for them, it’s less likely people will get the shot. It’s harder to get to a doctor than it is to a pharmacy and those discussions leave things up to personal and doctor’s choice.
On the flip side, it’s easy to get to a pharmacy and easier to do what you’re told rather than think it through. So when the ACIP wants to take away discussion, what they’re really saying is they want to minimize informed consent. They don’t want to encourage doctors and patients to discuss vaccines; they simply want people to get the shots. “Shared” decision making is the opposite of public health — it is primary, individual health care.
By going down this path, the ACIP is creating a less safe situation and increasing the chance for vaccine injury or death by ignoring individual circumstances and making directives one-size-fits-everyone-who-will-comply. They know people assume that a shot is safe if it is recommended. This ACIP trend is right in line with a federal less-is-more approach to informed consent around vaccines detailed in our meningitis article — less information leads to more consent. The CDC doesn’t want to “add cognitive work.”
One ACIP member summed it up well: “We know shared clinical decision making doesn’t work.” Doesn’t work for what? Doesn’t work for informed consent? Doesn’t work for individual choices and concerns? Doesn’t work to protect our religious freedoms? The only answer is that it doesn’t work to increase vaccine use.
Pneumococcal discussion
Imagine suggesting something you’re against? This was the predicament for the chair of the pneumococcal working group, Dr. Jamie Loehr.
The pneumococcal vaccine is currently recommended for infants at 2, 4, 6, and 12 months, and then again at age 65. Now, it will be recommended for adults starting at age 50.
The 2024 schedules have three pneumococcal vaccines: PCV15 (Vaxneuvance), PCV20 (Prevnar 20), and PPSV23 (Pneumovax 23). A new vaccine, PCV21 (CAPVAXIVE) was approved by the FDA on June 17 and recommended by the CDC on June 24, 2024. PCV21 is intended to target strains that cause disease in adults. For this reason, there’s no plan to get this on the childhood schedule, but it will be added to the adult schedule.
If this sounds confusing, it’s because it is. This is a common complaint and one that the ACIP is acutely aware of. Much of the discussion was about simplifying the recommendations, which is always with the intent to move more shots. ACIP members agreed this has been a confusing recommendation, but there are two new vaccines expected in 2025, so they expect recommendations to change again. These vaccines change so much because they keep adding and swapping strains.
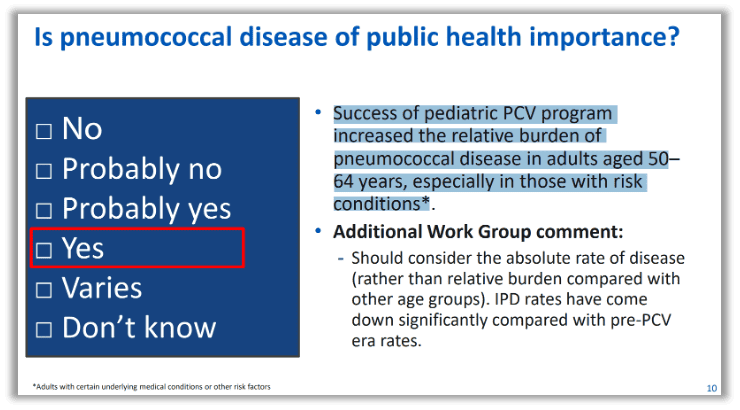
Why was there an ACIP working group to look at lowering the age of recommended adult pneumococcal vaccine? Because since we started vaccinating infants, adults are more likely to be diagnosed with pneumococcal disease. Tucked away on a slide justifying the shot, we’re told the “[s]uccess of pediatric PCV program increased the relative burden of pneumococcal disease in adults aged 50-64 years, especially in those with risk conditions.” So when vaccinating kids increases adult illness because the can is kicked down the line, the answer is vaccinate again when you’re older!
The pneumococcal vote was the only one that was not unanimous. The consensus in the working group was to lower the age-based recommendation to 50 from 65. However, chair Jamie Loehr, an ACIP veteran, and some unnamed others, were not on board with that because he didn’t believe everyone needed it and because of several unanswered questions.
Also of note was discussion of a “potential” signal for Guillain-Barre Syndrome (GBS) following vaccination with PCV20 (Prevnar).1
Meningococcal discussion
Currently there are two meningococcal shots on the schedule, one covers four strains, and is recommended, and the other covers only one and was limited to certain circumstances. But that’s changing as it is now recommended for certain kids and encouraged for healthy kids.
The meningococcal vaccine that includes four strains (A, C, W, Y) is still recommended at ages 11 and 16 years, but now there’s a recommendation for an additional meningococcal shot covering one more strain (B) (Bexsero) for kids 10 and older who are at higher risk of B meningococcal, as well as a new directive for parents and doctors of healthy kids aged 16-23 to consider adding the two-dose series for B. The advice for a MenB shot is not a recommendation yet, but instead the ACIP wants doctors and parents to have “shared clinical decision making” to talk about the possibility of getting the extra shots.
Summary of changes to both schedules
The October ACIP meeting is traditionally when the group updates their schedule. Even though last year they changed the schedule to include a blank page for updates throughout the year, they still met to discuss and rubber stamp updates.
- Influenza, COVID, polio, TD, Hib, RSV, and dengue were updated for current recommendations.
- Note that for COVID it is specifically noted now to not mix brand-name products for anyone under 6 months or for those who are immunocompromised.
- COVID notes include a new definition for an unvaccinated person as someone who has never gotten one. This is a change from definitions over the last four years that included people who were not “up to date” as “unvaccinated.”
- Clarification was made to not recommend pneumococcal or certain hepatitis B vaccines during pregnancy due to “limited data,” on seasonality and administration of RSV or nirsevimab to pregnant women or their babies, and MMR travel recommendations were updated.
- Meningococcal B changed from only high-risk recommendations to “shared clinical decision making” on the childhood schedule.
- Pneumococcal vaccine recommendation age lowered for adults.
- Updated to include recommendations for vaccines for adults with certain organ transplants
- Language and notations were edited to “harmonize” bring into accord) the adult and childhood schedules.
What else did ACIP cover?
As noted in our last update, the ACIP has a working group examining evidence on whether a one-dose recommendation should be used instead of two for the HPV vaccine Gardasil. More importantly, they are considering whether their recommendation should be lowered from age 11 to age 9 for girls and boys, because the FDA licenses it for kids that young.
Influenza, avian flu, mpox, and chickengunya vaccines and outbreaks were discussed, reiterating info without providing much more insight.
Notable agency update
The Health Resources and Services Administration (HRSA), which oversees our vaccine and countermeasure injury compensation programs, noted that a report was issued in August 2024 by the National Academies of Sciences, Engineering, and Medicine (NASEM) that will be used in the CICP and VICP that examined causal relationships between shoulder injuries and vaccines, as well as COVID-19 side effects.2 We will watch to see how this could change the claims and awards for victims of vaccines and EUA products.
Also, notably, work on the Vaccines National Strategic Plan 2026-2030 has begun. There will be listening sessions in the coming weeks and SHF will keep you updated when more information is available. Stay tuned for action items on the horizon!
Key takeaways
- A pregnancy schedule, with added vaccine recommendations (GBS is in the works) is on the horizon.
- Every schedule is set up to expand like an accordion. Votes are anticipated for more pneumococcal shots in 2025.
- Every ACIP meeting for the last year or more has included calls from the ACIP or the public during comments for a Vaccines for Adults federal program which would parallel federal purchases of products on the childhood schedule mandated through the Vaccines for Children (VFC).
- The Vaccines National Strategic Plan is being updated for 2026-2030 — look for information and action items to come from SHF!
Stay vigilant, friends. SHF is here to keep you informed and let you know when our voices can make the most difference.